Reconciling doctor as clinician and doctor as entrepreneur: the information practices and identity work of early career surgeons
Shona Gallagher and Michael Olsson
Introduction. The study examines the information practices of early career surgeons. Methodologically, it uses critical discourse analysis in conjunction with two social constructivist theories, Lloyd's information practices and Alvesson and Willmott's identity regulation and identity work.
Method. In-depth, semi-structured interviews were conducted with early career surgical specialists transitioning from accredited training to private practice. Participants were asked how they navigated two professional contexts in constant tension: doctor as clinician and doctor as entrepreneur.
Analysis. Interview transcripts were reviewed by an inductive process approach of constant comparison.
Results. Participants engaged in different information practices whilst functioning in different professional contexts. They described the difficulty of being caught between two worlds and revealed encounters with taboo subjects surrounding surgical fees. The information practices of participants not only involve problem solving or information acquisition but are also inextricably linked to the construction of their professional identity.
Conclusions. The findings suggest that critical discourse analysis is a useful tool for exploring the organisational control of professions. It suggests a strongly entwined relationship between information and identity practices and raises questions about the value of everyday life as a library and information science research concept.
Introduction
This article reports the findings of a study of the information practices of early career surgeons transitioning from training to working in private practice. In particular it focuses on the information practices participants use when trying to make sense of their role as business managers. Findings show that the information practices of early career surgeons prompt them to review what it means to be a good doctor.
The study is based on in-depth interviews conducted with six early career surgeons. Australia has a two tier health system offering public and private care. Surgeons work in both these environments. There is professional prestige attached to a public teaching hospital appointment which traditionally translates to a business advantage. These positions are usually held for the duration of a surgeon’s career. Hence, there is fierce competition among early career surgeons for a public hospital appointment, particularly a public teaching hospital appointment. Competition is further fuelled by a decreasing number of public teaching hospital positions, an increasing number of medical graduates, and lengthier training periods. Only a small number of surgeons derive 100% of their income from the public sector. The majority earn most of their income in the private sector and are effectively self-employed (Royal Australasian College of Surgeons, 2016). Australia is the only country in the Organisation for Economic Co-operation and Development (OECD) that allows doctors complete price freedom (Paris, Devaux, and Wei, 2010).
When working in private practice, surgeons are simultaneously engaged in two roles in constant tension: doctor as clinician and doctor as entrepreneur. Of particular interest to this study is the contrast in the training surgeons receive for these two roles. To qualify as a clinician they engage in an average of twelve years of training, must pass fellowship exams in order to be admitted to the surgical college which trains and regulates their specialty, and must demonstrate continuous engagement in professional development throughout their career. In their role as doctor as entrepreneur they receive no formal training and are only offered limited, optional workshops from their governing professional colleges. The Australian Competition and Consumer Commission (ACCC) Act of 2010 prohibits surgeons from discussing fees with one another unless they practise through the same legal entity (Australian Competition and Consumer Commission, n.d.).
Participants in this study described encountering taboos when they tried to approach senior colleagues for guidance and information about setting fees and running a private practice. Participants also described great difficulty in navigating the tension between the two roles of doctor as clinician and doctor as entrepreneur. Reflecting upon these tensions led many participants to question what it means to be a good doctor and to review the type of doctor they wanted to be. This indicated that participants reviewed their professional identity as a result of their information practices.
In order to better understand professional taboo topics and identity construction, the original research question exploring the information practices of early career surgeons navigating the two contexts of doctor as clinician and doctor as entrepreneur was expanded to the following;
- How does the surgical profession shape the information practices of surgeons?
- What is the role of identity construction in the shaping of their information practices?
Conceptual framework
The present study builds upon information practice research which focuses on the role of social practices in shaping the behaviour of individuals (Lloyd, 2010; McKenzie, 2003; Savolainen, 2007). Lloyd defines information practices as:
An array of information-related activities and skills, constituted, justified and organized through the arrangements of social site, and mediated socially and materially with the aim of producing shared understanding and mutual agreement about ways of knowing and recognizing how performance is enacted, enabled and constrained in collective situated action (Lloyd, 2011, p. 285).
The present study also joins other library and information research which engages with critical discourse analysis as both a methodology and a theory in the Foucauldian tradition (Johannisson and Sundin, 2007; Olsson and Heizmann, 2015). Critical discourse analysis has been described as the link between power and discourse (Clegg, 1989; Grant, Iedema, and Oswick, 2009; Talja, 1999). It draws upon the work of poststructuralist theorists such as Bourdieu, Derrida, Foucault and Lyotard to argue that the actor-agent is simultaneously influenced by and plays a central role in power relations (Fairclough and Wodak, 1997). To illuminate these power relations, critical discourse analysis uses various forms of textual analysis (Fairclough, 1992).
Foucault's work has been most influential on informing critical discourse analysis. For Foucault, language in the form of discourses constitutes object and subjects. Discourses arrange the social world in ways that inform social practices. These social practices constitute forms of subjectivity in which human subjects are given what is perceived to be a rational, self-evident form that manages who they are and what they do (Foucault, 1976, 1980; Grant et al., 2009).
The manner in which Foucault influences critical discourse analysis acknowledges the importance of the relationship between discourse and power and makes it an attractive proposition for information practice researchers. Information practice researchers Heizmann and Olsson (2015, p. 757) note that 'Collaborative ways of interacting among peers are as much the product of specific power relations as excessive knowledge hoarding and influencing tactics.'
The present study focuses attention on the relationship between information practices and professional identity. Academic definitions of profession and professionalism have been debated in recent decades among management, organisation, sociology and medical education scholars (Birden et al., 2014; Saks, 2012). Traditionally, professions are seen as institutional entities governed by codes of ethics and professing commitment to competence, integrity, morality, altruism and the promotion of the public good within their expert domain.
Foucault (1973, 1979) adopts a more critical approach centred on governmentality. In this view, the professions are seen as social constructions of power/knowledge involving the 'institutionalisation of expertise', in which professional bodies, teaching institutions, hospitals etc. become central actors in the discursive landscapes of the professions with which they engage. Individual members of a profession must construct their own professional knowledge and identity in the context of the rules and norms defined and policed by these institutions. This discourse analytic way of constructing the nature of the professions has strongly influenced the present study.
Previous information science studies have explored the information behaviour and information practices of medical professionals when participants are functioning in the role of doctor as clinician. Information behaviour studies have typically focused on the information seeking behaviour of surgeons and physicians (Booth, Carroll, Papaioannou, Sutton, and Wong, 2009; Clarke et al., 2013; Grant, 2017; Ward, Stevens, Brentnall, and Briddon, 2008). Discursive studies involving doctor-patient relationships have been conducted by information practice researchers; however, the focus of these studies has been on the information practices of patients rather than those of medical practitioners (Andsager and Powers, 2001; Dervin, Harpring and Foreman-Wernet, 1999; Godbold, 2012; McKenzie, 2002, 2003; Tuominen, 2004). Bonner and Lloyd (2011) studied the information practices of renal nurses performing clinical responsibilities and Johannisson and Sundin (2007) explored discourses at work in the nursing profession which shape knowledge claims.
In their study of health care and other types of professionals, Leckie, Pettigrew and Sylvain (1996) acknowledge different roles, associated tasks and information behaviour among professionals but do not take a discursive approach. Their definition of a health care system does not include the business, financial, policy development, governance or regulatory elements of the system. The Leckie et al. study, and others previously mentioned here, note that medical professionals use a variety of information sources when addressing their information needs. These sources are multi-faceted and range from authorised guidelines and academic journals to seeking the opinion of more experienced colleagues (Leckie, et al., 1996).
Iedema, Degeling, Braithwaite, and White's 2004 study of doctor-managers explores how doctors navigate the tensions between their profession and organisation, specifically the public hospital and area health service that employs them. They conceptualise doctors as functioning in the roles of doctor as clinician and doctor-manager. The study explores language within interview data as a means of identifying discursive boundaries used by doctor-managers to mitigate their reluctance to impose organizational rules upon fellow clinicians. Iedema et al.'s study engages with one doctor-manager participant in each of three formal management settings of similar context. In each of these settings the doctor-manager is a senior member of their profession, functioning as an employee of the broader hospital research site. The researchers acknowledge that 'despite these differences, each setting induced sacred, front-stage talk, rather than profane, off-the-record talk' (Iedema et al., 2004, p. 28). In contrast to that study, the interview data collected in the present study includes candid talk, direct acknowledgement of the difficulty of navigating between the two worlds of clinical and entrepreneurial work, and more detailed descriptions of how participant information practices are shaped by their profession.
Shunning discussion of particular subjects is a form of information avoidance and is the result of negative emotions giving rise to anxiety and fear (Chatman, 1992; Savolainen, 2014). Sociologists broadly agree that taboo subjects and activities current in any society tend to be significant to the social order. They are usually avoided in order to avoid causing embarrassment or offence. Within library and information science, the topics of shame, secrecy and stigma have been most thoroughly explored by Chatman in her studies of information poverty. Findings in our study suggest similarities between the information landscape of early career surgeons searching for information relating to the business side of their practice and Chatman's information poor participants. This raises the surprising possibility that early career surgeons are similar to Chatman's elderly retirees, janitors and single mothers in regard to being made and kept information poor by the accepted discursive practices and social norms operating within their profession. Chatman (1996) claims that information poverty is reinforced among information poor groups who identify as outsiders 'by neglecting to accept sources of information not created by themselves' (p. 193). The social nature of taboos and the means by which they are enforced demonstrate the importance of exploring the social aspects of information practices in order to understand the context of any individual's actions.
Identity and professional identity have previously been studied by information science researchers. Given (2003) used social positioning theory to explore the social construction of stereotypical student identities and the ways that mature students interact with available discourses and the implications for their information behaviour. Hicks (2014, 2016) studied the professional identities of librarians with a focus on professional identity construction surrounding library advocacy and the value of exploring professional identity to provide insight into why professionals behave the way they do. Both studies acknowledge the interconnection between identity construction and information practices. The present study continues this exploration.
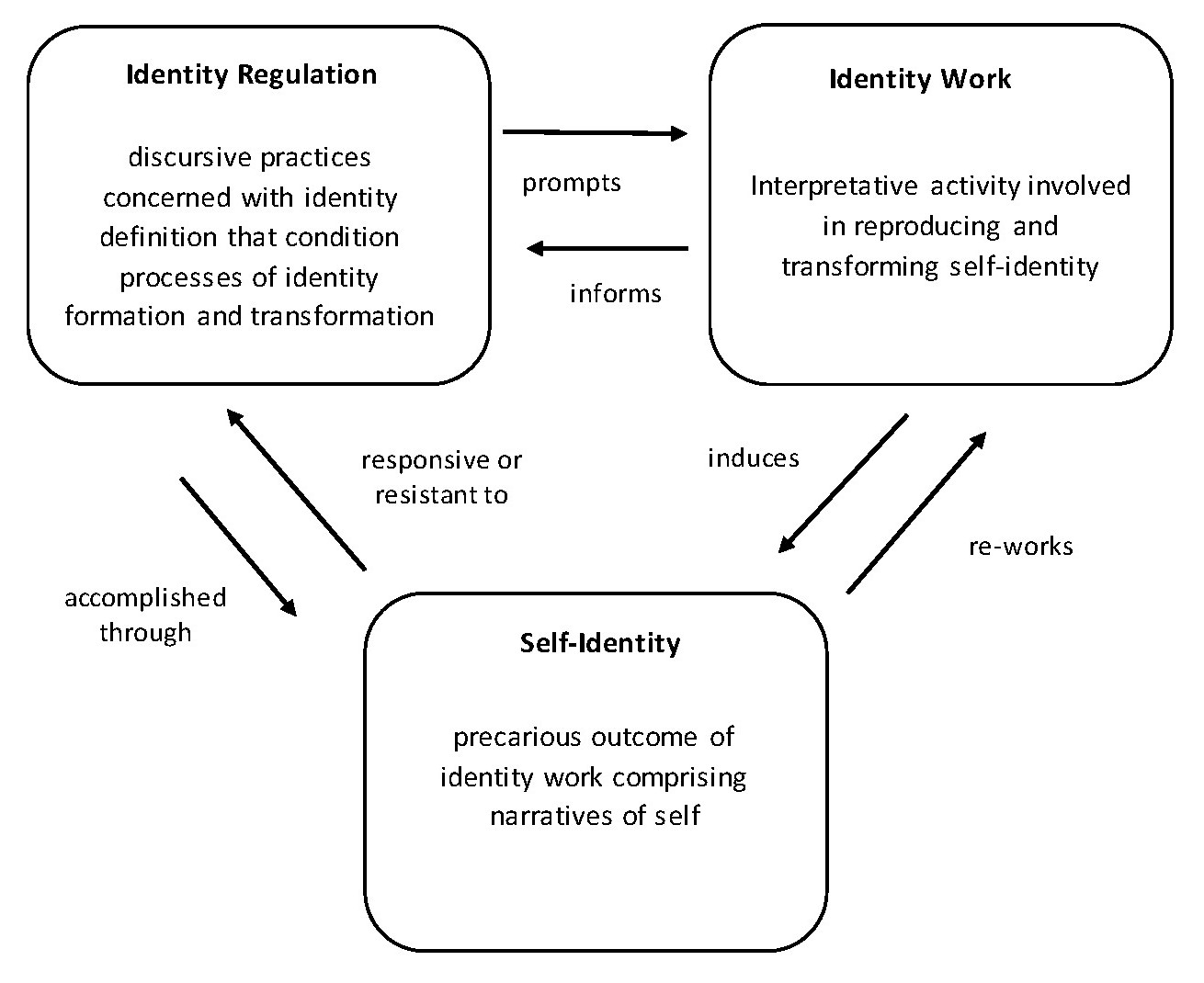
Identity research is now considered 'a critical cornerstone' (Brown, 2015, p. 22; Cerulo, 1997, p. 385) in contemporary sociological and social psychological theorising (Elliot, 2001; Gleason, 1983). The identity theory enlisted in this study is Alvesson and Willmott's (2002) concepts of identity regulation and identity work, jointly referred to here as identity practices. Alvesson and Willmott describe identity regulation as a form of organisational control which incorporates the intentional and unintentional action of management to influence employees' self-constructions of identity. One of the nine key modes of discourse listed in their theory of identity regulation is 'knowledge and skills'; 'knowledge defines the knower: what one is capable of doing (or expected to be able to do) frames who one "is". Education and professional affiliation are powerful media of identity construction' (Alvesson and Willmott, 2002, p. 630). Identity work is the fluid and continuous process of accepting or rejecting identity regulation (see Figure 1).
Method
Gallagher conducted semi-structured in-depth interviews with six early career surgeons transitioning from training to establishing their careers in private practice. The participants, all Fellows of the Royal Australasian College of Surgeons (RACS), came from two surgical specialties; general surgery, and plastic and reconstructive surgery. Four participants were female, two were male. Four worked in a combination of private and public practice and two worked exclusively in private practice. The average age was thirty-seven years.
The interviews ranged from fifty-five to eighty-six minutes long with an average length of seventy-two minutes. After general questions about why they became a doctor, participants were asked to describe how they navigated the dual roles of medical practitioner and business operator. They were asked how they set fees, where and to whom they turned when they had questions or needed help, and whether or not they considered themselves entrepreneurs.
Gallagher recruited participants through several purposive sampling methods, including criterion sampling whilst attending the 2018 RACS Annual Scientific Meeting and a variation of criterion snowball sampling. Participants had to meet the following criteria:
- Fellow of the Royal Australasian College of Surgeons (RACS) or equivalent surgical training college;
- Have been admitted to RACS within the past five years;
- Have entered or be in the process of considering entering private practice;
- Have completed their specialist surgical training in Australia.
The interviews were recorded, transcribed verbatim style and annotated by Gallagher in regard to professional jargon. Gallagher has worked with surgeons on a daily basis for more than twenty years in her capacity as co-director, co-founder and co-owner of a private surgical practice attached to a Sydney public teaching hospital. Gallagher analysed the data in consultation with Olsson using an inductive approach of constant comparison.
Names of the participants have been changed to protect their identity. Pseudonyms have been chosen from the list of most popular boys and girls names in Australia in 1983, the year of participants' birth based on their average age.
Findings
Participant interviews typically progressed from straight forward, relaxed narratives describing information practices in the role of doctor as clinician to fraught and emotional narratives describing the difficulties and obstacles encountered in the role of doctor as entrepreneur.
Patterns in accounts of information practices
Participants provided extremely rich accounts of their information practices. They described great difficulty navigating the two roles of clinician and entrepreneur. These difficulties were sometimes matters of practicality, for example, an inability to find an authoritative or definitive source. At other times, the difficulties were ontological as participants tried to balance expectations with reality.
Practical difficulties: no official guidelines
Descriptions by participants of their information practices while functioning in the role of doctor as clinician were unsurprising. They were consistent with the evidence-based pedagogy of their training and usually included talking to colleagues and referring to academic journals. Here Amanda responds to being asked to what or whom she turns when she has questions about the clinical aspects of her practice:
Clinically, I read journal articles. I look up, I look up a journal article because I think journal articles are - all my colleagues internationally are, like, there for me. Like they – so here's my series of a thousand patients for this operation, so if I'm ever not sure, I just read, which is what we used to do when we were training, right, because you can't call your boss for everything and then, then if you ask one person, you're limited by their experience, whereas if you internationally seek data then that's better, you're researching it and I think, like, you're a strong believer of that. (Amanda)
Amanda searched for similar resources when she tried to address her information needs in the role of doctor as entrepreneur. In the following excerpt she describes her experience trying to determine the best way to set her fees:
So I called the College [RACS], 'Okay, what are your guidelines about setting up a practice?' and they said, 'It's our job to train you to be a surgeon. It's not our job to train you to run a practice.' (Amanda)
This account is also typical. Participants described starting the process of answering their questions by searching for formal guidance and instructions. They described searching for resources online and over the phone by contacting their training colleges and professional societies. They also described attempting conversations with their more experienced colleagues. As participants exhausted formal information sources, participants turned to informal sources:
So basically, we Googled, like the top – like five average surgeons in Sydney, some of which published their prices and I went, 'Okay, let's go half to 75% of their fee'.... I haven't had a guideline. (Amanda)
Most participants described engaging with financial advisors, lawyers and accountants for professional advice but not in regard to setting fees. Typically participants used their personal experience as paying customers of other trades and services to justify their fees. Comparisons included plumbers, other trade professionals, and event managers:
And so, you – you're really stuck, you're really stuck, so you do spend some time having a crisis of conscience trying to figure out, how to go about things, and then you kind of spend time thinking about, 'How I'm going to – how, how I rationalise this in my head?' and then, eventually, you call a plumber to come and quote you for something at home or you ask a tradie to come for whatever reason and you – your jaw drops when they tell you the price that they charge, and then you think to yourself, You know what? I'm actually dealing with people's health. Like I'm actually trying to extend their lives, relieve their pain, you know, suffering. (Christopher)
The locum: learning while working in another doctor's practice
All but one of the participants in this study had worked as a private locum or were employed at the time of the interview as a locum in another doctor's private practice. In a typical locum position, the locum does not work in the practice at the same time as the doctor who employs them. The participants described learning a great deal about private practice from their locum experiences, including clinical and business practices of which they did not approve. Their descriptions of interactions with practice staff also revealed status distinctions between themselves and individuals they did not consider to be performing clinical functions. These signals of self-identified hierarchical location are an example of identity work. They are also signals of knowledge ranking. In the description below the participant asserts her superior clinical knowledge to discount a request from a non-clinical manager:
I had someone come to me and tell me I had to cut down my – the length of my letters and I find that really difficult as well, so. That it was taking them too long to go through, to edit my letters, and that GPs [general practitioners also known as primary care physicians] didn't want long letters and that I should therefore cut them down and put it as bare bones and that didn't sit very well with me …. So, it came down from – so, the person who spoke to me about it was sort of a practice manager, but not. She like was in the middle between the surgeons and the practice manager. And it had come from one of the surgeons. There's like the chief surgeon, I guess, in the practice. And I thought, I'm not your lackey… So, it really riled me up and that was the second defining moment where I said, 'This is not – this practice is not for me'. (Jennifer)
Billing practices can be quite complex: for example, knowing which item numbers from the 5,700 different services listed in the Medicare Benefits Schedule (MBS) to use and how much to charge. Medicare is a publicly funded universal health care system that gives Australian residents access to healthcare. It covers part or all of the cost of services itemised in the Medicare Benefits Schedule. Private health insurance rebate payments are calculated according to the Medicare Benefits Schedule. Bulk billing is a term used to describe the practice of doctors choosing to be paid the minimum fee by billing the government directly. In the period 2017-2018 less than one-third of medical specialists bulk billed their patients (Australian Government Department of Health, 2018). The participants who worked as locums described learning about billing practices directly from practice staff:
I was talking to the practice manager there, who's like, 'This is what people would do.' (Jessica)
Taboos: 'You're just money hungry'
When formal societies and guidelines failed to provide information about patient fees some participants tried turning to senior colleagues. These participants described awkward and unproductive conversations which made them feel they were raising forbidden topics:
In fact, it's frowned upon if you try and work out how to open up a practice. It's frowned upon, 'oh you're just money hungry'. (Amanda)
Participants also described indirect, informal efforts by senior colleagues to influence their behaviour:
I follow suit with what the practice is charging, uhm, and – but I do have, uh, the ability I guess to bulk bill or, uh, try to reduce the consult fee and I do that frequently. Uhm, if I over-reduce fees then, you know, sometimes I get sort of, you know, a hint saying, you know, uhm, what are you doing, sort of thing. (Michael)
These are both examples of informal organisational control. As participants engaged in information practices relating to the role as doctor as entrepreneur they frequently met with disapproval from senior colleagues. This indicates a set of information barriers governed by social norms rather than a lack of available information. Based on her experience in the health sector Gallagher suggests that disapproval expressed by senior colleagues may be the result of a number of factors. These include: deflecting embarrassment about how much they charge; deflecting embarrassment about the lack of rigour behind their pricing structure; deflecting fear of appearing poorly informed in front of junior colleagues; deflecting fear of discovery of unethical billing practices; and deflecting fear of accusations of collusion by the ACCC. The majority of these factors relate to reputation protection, itself a form of identity work.
The should count: constant reviewing of obligations and expectations
Participants used the word should one hundred times in 433 minutes of interview time.
I tend to undervalue myself and I find it really hard to sometimes see that I should be charging patients. (Jennifer)
So I had this dilemma, do I call myself a cosmetic or a reconstructive or-- so I've gone with cosmetic and reconstructive plastic surgeon, like, so you try and combine it all when, should I just stick to plastic and reconstructive surgeon? (Ashley)
The word should indicates a sense of obligation, duty, or correctness. Obligations represent written and unwritten rules of society, the prevailing discourses that shape our behaviour. Counting participant use of the word should provides this study with a blunt empirical measure of the sense of dilemma participants expressed and narrated as they struggled to reconcile tensions. Amanda used should thirty times, once every two and a half minutes, closely followed by Ashley and Jennifer. Michael used should seven times, once every twelve minutes, and Christopher used should twice in fifty-five minutes. Jessica used should thirteen times in sixty-three minutes. Each time a participant used the word should they were referencing a social norm. These norms govern their information practices and identity practices by providing rules for what they ought to know while at the same time preventing them from stepping outside the rules to acquire information they may need. In-depth linguistic analysis of interview data presents an opportunity for further study and suggests gendered behaviour although the researchers caution that the stage of transition of participants between training and practice may be another factor at play. Women represent 40% of all Australian medical practitioners but only 11% of surgeons (Australian Institute of Health and Welfare, 2016; Liang, Dornan, and Nestel, 2019). This puts female surgeons in an extreme minority position with implications for cultural practices in the professional community.
Navigating tensions between doctor as clinician and doctor as entrepreneur
Participants described various ways in which other members of their profession attempt to shape their behaviour. Amanda describes how her efforts to be a good surgeon are a complex mix of clinical, technical, personal and ethical skills which develop as a result of a range of information practices. Her self-described process of realisation is itself the result of information practices as she advances beyond the rules and regulations she learned as a novice and proceeds to questions the decision-making tools she has been taught to use by her senior colleagues. Amanda also refers to doctor as clinician and doctor as entrepreneur as central to the good surgeon identity demonstrating simultaneous engagement in multiple discourses. She also describes indirect efforts made by members of her profession to shape her identity, specifically whether or not surgeons should be nice. Furthermore Amanda describes her agency in resisting these efforts and expresses triumph is distancing herself from her peers, an example of micro-emancipation:
I think if you don't care about the patient then I doubt that you'll ever be a good surgeon. So people who are good technically but just don't, don't spend the time, don't spend the effort, try and get the patient in and out and give them a substandard result because it's a financial decision, not a, 'I'm going to care about this person' decision. So we should do more to attract nice – is the word nice? It's not. It's more compassionate, people have empathy and we lack that in surgical training. Like I got told during my training that I'm too nice. So I actually got pulled up for a couple of times to say, you know, 'You are too nice', like multiple times actually, even general surgery like, 'You're too nice to be a surgeon'. I'm like, 'What does that mean exactly?' Is it because I'm courteous to my colleagues or my juniors or because I'm polite to my patients? What does too nice mean? And I still don't understand what that means, because guess what, the patients love it. (Amanda)
Another indirect attempt at shaping behaviour is expressed by Christopher:
While you're training there is a certain tone attached to private surgeons. There's an undercurrent, while you're training, the feeling comes through that you really – the only way you even made it in life or made it in surgery, is to have a public hospital appointment. (Christopher)
His account describes the prestige attached to public teaching hospital positions. Surgeons with public teaching hospital appointments control the surgical specialty training schemes and examine trainees for their final exams. They typically engage in more complex medical cases than their colleagues working solely in private practice and are eligible for academic positions and affiliations. Public teaching hospitals have relationships with university medical schools and research institutions including salaried surgical academic appointments. Teaching hospital positions are considered profitable because the associated prestige of technical superiority attracts private referrals to the private practices of these surgeons. There is also a moral superiority associated with caring for the general public and teaching future generations of medical practitioners. Christopher indicates how his failure to achieve a teaching hospital appointment has long term implications for information practices throughout his career:
If I go to a conference and you talk to your colleagues, you're almost looked down upon; in fact, you are looked down upon, you know, 'Where do you work?' 'I work here [private practice] but I don't have a public [hospital appointment]', 'Oh, oh, okay.' 'So…' and they turn around and look at someone else. That's how, that's how it works with the College of Surgeons. Christopher)
The insider versus outsider social positions of surgeons with public hospital appointments versus those without suggests the existence of communities of practice that are bounded by social position and professional identity.
The extent of the distance placed by members of the surgical profession between the roles and identities of doctor as clinician and doctor as entrepreneur is expressed by Ashley:
I became a surgeon because I didn't want to be a business person. If I wanted to do business, I would've gone into business. You know? And you're sort of forced into these… positions. (Ashley)
Rejection of the identity of entrepreneur
All participants were asked if they considered themselves entrepreneurs or medical entrepreneurs. All participants asked for a more specific definition and were instructed by the interviewer to provide their own interpretation. Michael, a plastic and reconstructive surgeon, was the only participant who did not entirely reject the identity of the entrepreneur. He talked through various interpretations of doctors as entrepreneurs including cosmetic surgeons who run large practices which administer a lot of cosmetic injectables to patients, an identity he rejected, and doctors as entrepreneurs who develop innovative technology:
If I do have an idea (about implant developments) then I could see myself potentially developing that idea at some stage but that would be something that I do parallel with my clinical work (Michael).
This distancing behaviour was also captured to various degrees within interview data when participants described how they engaged other people to perform the more entrepreneurial aspects of their work:
I forgot to tell you something. So my husband helps me a lot. I forgot to mention him. So he, he's a XXXXXX and a few – about a year ago, six months ago, he, uhm, quit XXXXXX and he's doing an MBA. So he has helped me a lot with Google Ads and social media and stuff like that because he – like it's part of MBA, they teach them these things... So he's been really good actually. So he has done – that's what I forgot to tell you, so he's done a lot of that kind of business side. So he doesn't have an ethical dilemma because he's not direct, he's not me. (Amanda)
In this excerpt Amanda describes outsourcing not only her information practices but also her ethical responsibility. This has implications for the social responsibilities of her profession. It suggests that her efforts to protect her self-identity as a good doctor include choosing to be information poor about the business aspects of her practice.
Discussion
This study focuses on professionals who are experiencing a significant transition in their career. In focusing on this group the study explores the different information and identity practices these individuals use when they function in two professional roles, doctor as clinician and doctor as entrepreneur. All participants described similar experiences: as they engaged in various information practices in order to address their information needs regarding the business aspects of private practice, they were prompted to perform identity work. Initial analysis of the findings indicates a number of information and identity discourses. This suggests that identity, information and constructions of power and authority are entwined and warrant further exploration by information science researchers.
Rather than the individuals' information practices and identity work being entirely ruled by prevailing discourses, initial findings reveal micro-emancipations consistent with Alvesson and Willmott's model of identity work. This suggests that the 'battle for truth' (Foucault, 1980) takes on new levels of complexity, along with the possibility of greater individual agency, when viewed from the level of the practices of the individual practitioner rather than the more macro-sociological level more usual in the Foucauldian tradition. These micro-emancipations involved both intellectual and emotional labour.
The emotional labour at the heart of navigating these discursive boundaries also has underexplored implications and may, as suggested by Ahuja and colleagues, 'express a sense of disillusionment that leads to the constitution of dejected professional identities' (Ahuja, Heizmann, and Clegg, 2019). The longer term implications of the relationship between identity work and information practices are yet to be explored by this study and library and information science in general. The cultural divide between public and private surgeons identified in this study suggests the existence of communities of practice that limit ongoing information practices on the basis of professional identity.
Another area for further research arising from this study is exploration of the interaction of information practices and identity practices in relation to professional taboos. Different approaches to billing by individual surgeons reveal information and identity discourse boundaries within the profession. This suggests information and identity discourses may reinforce boundaries of informal communities of practice within the surgical profession and how these communities of practice influence information practices across different professional contexts. Members of communities of practice which are strongly discursively bounded may meet Chatman's criteria for being information poor. Chatman's conceptualisation of insiders and outsiders raises questions as to how discursive professional information and identity boundaries impact the construction, adaption and integration of medical treatment and technology innovations, health policy development and the delivery of patient care.
According to Larson (1977), 'Because of their unique knowledge and skill sets, society grants professionals higher levels of prestige and autonomy than it grants non-professionals' (p. x). In line with Kuhn (2009) and Pratt, Rockman and Kaufmann (2006), we also suggest that identity work is employed strategically to 'construct and maintain preferred versions of self' (Pratt, Rockmann, and Kaufmann, 2006, p.235). Next steps for this study include exploring the interaction of information practices with identity work by early career surgeons to reconcile the discrepancy between self-perceptions of performing as competent or proficient in the context of doctor as clinician while simultaneously performing as a novice in the context of doctor as entrepreneur. Public discourses that reinforce the social status of professionals and experts offer rich research possibilities within this study. Exploring the extent to which these discourses diminish or encourage professionals to maintain the status of novice within their professional information practices may provide insight into constructions of knowledge within the broader profession and contribute to an understanding of epistemologies of practice (Schön, 1992).
Conclusion
Our findings demonstrate the significance of critical discourse analysis in the context of information studies and introduces identity work and identity regulation as complementary theories.
Three key insights can be drawn from this study. Firstly, that information practices and identity work are social practices that advance one another. When individuals engage in information practices, they are prompted to review their self-identity. Similarly, the process of re-working their self-identity influences their information practices. This is most clearly captured in descriptions of the information practices and identity work conducted by participants as they battle with accepting or resisting the conflicting professional and societal discourses surrounding the capitalist economic expectations of marketing their clinical skills and promoting themselves as their own personal brand. The implications for patients, non-surgical health professionals, hospital administrators, policy makers, private health insurers, medical research institutions, medical instrumentation developers, the pharmaceutical industry and other health system stakeholders are yet to be explored.
Secondly, that the manner in which information science conceptualises professions and professionals warrants further investigation. Historically, library and information science practitioners have celebrated academic domains of scientific knowledge in a manner which may have resulted in a lack of recognition and exploration of the hidden curriculums at work in these domains and the ways in which these hidden curriculums shape the information landscape of professions. There are parallels here with Olsson's (2016) study of archaeologists, which also found a hidden curriculum relating to the embodied knowledge required for excavation in the field. What sets the two studies apart is that while Olsson (2016) found a supportive network of informal mentoring and associated information practices to support participants, this is notably lacking for participants in the present study. Instead, the current study suggests that some professions attempt to use social norms to control members by rendering them information poor and creating insider and outsider social positions.
Thirdly, that information in everyday life is a self-limiting research concept. This study demonstrates how individuals are capable of simultaneously engaging in multiple roles as well as multiple information and identity discourses. The intense, precarious information practices and identity practices of early career surgeons shows an ongoing state of individual reassessment to develop a cohesive sense of self. The intense work continues beyond the limitations of their professional training and the professional roles and tasks they execute and gives us insight into how the profession struggles to meet its legal and ethical obligations to general society.
Acknowledgements
The authors wish to thank the anonymous reviewers for their useful feedback. They would also like to thank Harriet Jordan for her invaluable assistance in copy-editing and coding the article
About the authors
Shona Gallagher is a doctoral candidate in information and knowledge management in the Faculty of Arts and Social Sciences at the University of Technology Sydney. Shona's research focuses on knowledge sharing within professions with a focus on the interaction of information practices, identity regulation and identity work. She can be contacted at: Shona.Gallagher@student.uts.edu.au
Michael Olsson is a Senior Lecturer in the School of Communication at the University of Technology Sydney. He has an MA (Information) and a PhD from the University Technology Sydney. Michael's research focuses on information practices in academic, professional, artistic and leisure communities, with a particular interest in embodied information practices. He can be contacted at Michael.Olsson@uts.edu.au
References
- Ahuja, S., Heizmann, H. & Clegg, S. (2019). Emotions and identity work: emotions as discursive resources in the constitution of junior professionals' identities. Human Relations, 72(5), 988-1009.
- Alvesson, M. & Willmott, H. (2002). Identity regulation as organizational control: producing the appropriate individual. Journal of Management Studies, 39(5), 619-644.
- Andsager, J. L. & Powers, A. (2001). Framing women's health with a sense-making approach: magazine coverage of breast cancer and implants. Health Communication, 13(2), 163-185.
- Australia Department of Health. (2018). Annual Medicare statistics 2017-2018. Retrieved from https://www1.health.gov.au/internet/main/publishing.nsf/Content/Annual-Medicare-Statistics (Archived at https://web.archive.org/web/20180817140341/https://www1.health.gov.au/internet/main/publishing.nsf/Content/Annual-Medicare-Statistics)
- Australia. Institute of Health & Welfare. (2016). Medical professionals in Australia in 2015. Retrieved from http://www.aihw.gov.au/workforce/medical/> (Archived at https://web.archive.org/web/20161105142042/http://www.aihw.gov.au/workforce/medical)
- Australian Competition & Consumer Commission. (n.d.). Fee setting by medical professionals. Retrieved from https://www.accc.gov.au/business/professional-services/medical-professionals/fee-setting-by-medical-professionals (Archived at https://web.archive.org/web/20180407133150/https://www.accc.gov.au/business/professional-services/medical-professionals/fee-setting-by-medical-professionals)
- Birden, H., Glass, N., Wilson, I., Harrison, M., Usherwood, T. & Nass, D. (2014). Defining professionalism in medical education: a systematic review. Medical Teacher, 36(1), 47-61.
- Bonner, A. & Lloyd, A. (2011). What information counts at the moment of practice? Information practices of renal nurses. Journal of Advanced Nursing, 67(6), 1213-1221.
- Booth, A., Carroll, C., Papaioannou, D., Sutton, A. & Wong, R. (2009). Applying findings from a systematic review of workplace-based e-learning: implications for health information professionals. Health Information & Libraries Journal, 26(1), 4-21.
- Brown, A. D. (2015). Identities and identity work in organizations. International Journal of Management Reviews, 17(1), 20-40.
- Cerulo, K. A. (1997). Identity construction: new issues, new directions. Annual Review of Sociology, 23, 385-409.
- Chatman, E. A. (1992). The information world of retired women. Westport, CT: Greenwood Press.
- Chatman, E. A. (1996). The Impoverished Life-World of Outsiders. Journal of the American Society for Information Science, 47(3), 193-206.
- Clarke, M. A., Belden, J. L., Koopman, R. J., Steege, L. M., Moore, J. L., Canfield, S. M. & Kim, M. S. (2013). Information needs and information-seeking behaviour analysis of primary care physicians and nurses: a literature review. Health Information & Libraries Journal, 30(3), 178-190.
- Clegg, S. R. (1989). Frameworks of power. London: Sage.
- Dervin, B., Harpring, J. E. & Foreman-Wernet, L. (1999). In moments of concern: a sense-making study of pregnant, drug-addicted women and their information needs. The Electronic Journal of Communication, 9(2), 3. Retrieved from http://www.cios.org/EJCPUBLIC/009/2/00927.html (Archived at https://web.archive.org/web/20160802114420/http://www.cios.org/EJCPUBLIC/009/2/00927.html)
- Elliot, A. (2001). Concepts of the self. Cambridge: Polity Press.
- Fairclough, N. (1992). Discourse and social change (Vol. 10). Cambridge: Polity Press.
- Fairclough, N. & Wodak, R. (1997). Critical discourse analysis. In T.A. van Dijk (Ed.), Discourse as social interaction. Discourse studies: a multidisciplinary introduction (Vol. 2, pp 258-284). Thousand Oaks, CA: Sage.
- Foucault, M. (1973). The birth of the clinic: an archaeology of medical perception. New York: Pantheon Books.
- Foucault, M. (1976/1990). The history of sexuality. Vol 1: An Introduction (Trans.. R. Hurley). London: Penguin.
- Foucault, M. (1979). Discipline and punish: the birth of the prison. New York: Vintage.
- Foucault, M. P. (1980). Knowledge: selected interviews and other writings. New York: Pantheon Books.
- Given, L. M. (2003). Discursive constructions in the university context: social positioning theory & mature undergraduates' information behaviours. New Review of Information Behaviour Research, 3, 127-142.
- Gleason, P. (1983). Identifying identity: a semantic history. Journal of American History, 69(4), 910-931.
- Godbold, N. (2012). Usefully messy: how people use rich, complex descriptions to make sense in online renal discussion groups. Chapter 3 in Social information research (pp. 43-73). Bingley: Emerald Group Publishing Limited.
- Grant, D., Iedema, R. & Oswick, C. (2009). Discourse and critical management studies. In M. Alvesson, T. Bridgman, and H. Willmott (Eds.), The Oxford handbook of critical management studies (pp. 213). Oxford: Oxford University Press.
- Grant, M. J. (2017). Ten years of reviews. Health Information and Libraries Journal, 34(1), 1-4.
- Heizmann, H. & Olsson, M. R. (2015). Power matters: the importance of Foucault's power/knowledge as a conceptual lens in KM research and practice. Journal of Knowledge Management, 19(4), 756-769.
- Hicks, D. (2014). The construction of librarians' professional identities: a discourse analysis/La construction de l'identité professionnelle du bibliothécaire: une analyse de discours. Canadian Journal of Information and Library Science, 38(4), 251-270.
- Hicks, D. (2016). Advocating for librarianship: the discourses of advocacy and service in the professional identities of librarians. Library Trends, 64(3), 615-640.
- Iedema, R., Degeling, P., Braithwaite, J. & White, L. (2004). 'It's an interesting conversation I'm hearing': the doctor as manager. Organization Studies, 25(1), 15-33.
- Johannisson, J. & Sundin, O. (2007). Putting discourse to work: information practices and the professional project of nurses. Library Quarterly, 77(2), 199-218.
- Kuhn, T. (2009). Positioning lawyers: discursive resources, professional ethics and identification. Organization, 16(5), 681-704.
- Larson, M. S. (1977). The rise of professionalism: a sociological analysis. Berkeley, CA: University of California Press.
- Leckie, G. J., Pettigrew, K. E. & Sylvain, C. (1996). Modeling the information seeking of professionals: a general model derived from research on engineers, health care professionals, and lawyers. Library Quarterly, 66(2), 161-193.
- Liang, R., Dornan, T. & Nestel, D. (2019). Why do women leave surgical training? A qualitative and feminist study. The Lancet, 393(10171), 541-549.
- Lloyd, A. (2010). Corporeality and practice theory: exploring emerging research agendas for information literacy. Information Research, 15(3), colis794. Retrieved from http://InformationR.net/ir/15-3/colis7/colis704.html (Archived at https://web.archive.org/web/2018*/http://InformationR.net/ir/15-3/colis7/colis704.html)
- Lloyd, A. (2011). Trapped between a rock and a hard place: what counts as information literacy in the workplace and how is it conceptualized? Library Trends, 60(2), 277-296.
- McKenzie, P. J. (2002). Communication barriers and information-seeking counterstrategies in accounts of practitioner-patient encounters. Library & Information Science Research, 24(1), 31-47.
- McKenzie, P. J. (2003). A model of information practices in accounts of everyday‐life information seeking. Journal of Documentation, 59(1), 19-40.
- Olsson, M. (2016). Making sense of the past: the embodied information practices of field archaeologists. Journal of Information Science, 42(3), 410-419.
- Olsson, M. & Heizmann, H. (2015). Power matters: Foucault's pouvoir/savoir as a conceptual lens in information research and practice. Information Research, 20(4), paper 695. Retrieved from http://InformationR.net/ir/20-4/paper695.html (Archived by WebCite® at http://www.webcitation.org/6dQGghNpT)
- Paris, V., Devaux, M. & Wei, L. (2010). Health systems institutional characteristics: a survey of 29 OECD countries (OECD Health Working Papers, 50). Paris: OECD Publishing. Retrieved from https://doi.org/10.1787/5kmfxfq9qbnr-en (Archived at https://web.archive.org/web/2018*/https://doi.org/10.1787/5kmfxfq9qbnr-en)
- Pratt, M. G., Rockmann, K. W. & Kaufmann, J. B. (2006). Constructing professional identity: the role of work and identity learning cycles in the customization of identity among medical residents. Academy of Management Journal, 49(2), 235-262.
- Royal Australasian College of Surgeons. (2016). Surgical workforce 2016 census report. Retrieved from https://umbraco.surgeons.org/media/1698/2017-05-26_2016-surgical-workforce-census-full-report_final.pdf
- Saks, M. (2012). Defining a profession: the role of knowledge and expertise. Professions and Professionalism, 2(1). Retrieved from https://doi.org/10.7577/pp.v2i1.151
- Savolainen, R. (2007). Information behavior and information practice: reviewing the "umbrella concepts" of information‐seeking studies. The Library Quarterly, 77(2), 109-132.
- Savolainen, R. (2014). Emotions as motivators for information seeking: a conceptual analysis. Library & Information Science Research, 36(1), 59-65.
- Schön, D. A. (1992). The crisis of professional knowledge and the pursuit of an epistemology of practice. Journal of Interprofessional Care, 6(1), 49-63.
- Talja, S. (1999). Analyzing qualitative interview data: the discourse analytic method. Library & Information Science Research, 21(4), 459-477.
- Tuominen, K. (2004). 'Whoever increases his knowledge merely increases his heartache': moral tensions in heart surgery patients and their spouses' talk about information seeking. Information Research, 10(1), 10-11 paper 202. Retrieved from http://InformationR.net/ir/10-1/paper202.html (Archived at https://web.archive.org/web/20180414155830/http://InformationR.net/ir/10-1/paper202.html)
- Ward, R., Stevens, C., Brentnall, P. & Briddon, J. (2008). The attitudes of health care staff to information technology: a comprehensive review of the research literature. Health Information & Libraries Journal, 25(2), 81-97.