Information Research
Vol. 29 No. 3 2024
Health information sharing – conceptual clarification and exploratory analysis in the context of mammography screening
DOI: https://doi.org/10.47989/ir293753
Abstract
Introduction. Information sharing is an important but under researched type of health information behaviour. In this study, we explore the characteristics of sharing behaviours, their reasons and determinants in the context of mammography screening.
Method. We conducted a two-wave online survey with N = 1,136 women. In the first wave, women saw an invitation letter to mammography screening and behavioural determinants were captured with established scales. In the second wave, women reported on their information behaviour between the two waves, combining standardized and open-ended questions.
Analysis. We performed qualitative content analysis and a stepwise logistic regression analysis.
Results. About one-fifth of the sample shared information on mammography between the two survey waves. Qualitative results revealed different causes and purposes of information sharing. Quantitative results showed that issue importance, opinion leadership and different types of information retrieval were related to information sharing.
Conclusions. The results shed light on two facets for the conceptual clarification of health information sharing: sharing in the sense of selecting and passing on information (cf. diffusion of information by opinion leaders) and sharing as the mutual exchange of opinions and experiences. Both facets should be considered to comprehensively examine health information sharing behaviours and their relation with informed decision-making.
Introduction
Information sharing is a crucial phenomenon in the context of health communication that describes the interpersonal transmission of health-related information typically gained from other sources such as mass media or health professionals (e.g., Crook et al., 2016; Fu et al., 2017). In addition, it can cover the disclosure of personal health information in interpersonal conversations (Huisman et al., 2020). This also concerns (intergenerational) sharing of one’s acute health status and family health history, i.e., chronic diseases and genetic dispositions (Ashida & Schafer, 2015; Binda et al., 2018), as well as the willingness to share health information in the context of eHealth (Naeem et al., 2022). Although the interpersonal exchange of information is a frequent and influential type of health communication, most information behaviour studies focus on rather unidirectional behaviours in terms of an individual’s seeking, scanning and avoiding of health information (Huisman et al., 2020). Hence, there is a need to further explore 1) characteristics of sharing behaviours, 2) their reasons and 3) determinants.
We study mammography screening as an exemplary use context. Mammography screening is the periodic examination of women without any symptoms with the aim of early detection of breast cancer. Our study is situated in Germany, where women aged 50 years and older receive an individual invitation letter with an appointment for a mammography every two years. Slightly more than half of the invited women in Germany participate regularly (Heinig et al., 2023). Women invited to the screening need to make an informed decision whether they want to participate (e.g., Abelson et al., 2018; Keating & Pace, 2018; van Agt et al., 2012). For their decision-making, research underlines the role of interpersonal communication (e.g., Lee et al., 2016; Nguyen et al., 2010) and sheds light on information seeking and scanning (e.g., Hornik et al., 2013; Shneyderman et al., 2016; Zhuang & Guan, 2021), but the role of information sharing or peer referral is seldom considered (Monrose et al., 2017; Southwell et al., 2012). We aim to bridge this gap by closely examining information sharing about mammography screening.
Health information sharing
Characteristics of health information sharing
In the health context, information sharing mainly refers to the fact that people may proactively pass on health-related information they received from various channels (mass media, campaigns, health fairs, health professionals) to other people (Fu et al., 2017; Monrose et al., 2017). In that, they may contribute to a collective pool of knowledge (Yang et al., 2022; Yang & Zhuang, 2020) or provide informational support (J. Liu et al., 2020) to those whom they believe have informational needs and/or a low health literacy (Crook et al., 2016). This kind of behaviour is different from health professionals’ occupational information sharing with patients. We examine everyday health information sharing as a voluntary behaviour that may stem from different reasons (see below).
Existing studies on health information sharing mostly focus on specific recipients (e.g., informal recipients, Huisman et al., 2020) or communication channels (e.g., social media, Döbrössy et al., 2020). In this study, we examine information sharing regarding a specific topic and in a certain situation, but with different recipients (e.g., informal and formal recipients) through various interpersonal and media communication channels:
Research Question 1: To what extent and with whom do women share information about mammography screening after reading an individual invitation letter?
Reasons for health information sharing
To date, very few studies have examined why people share health information. In an explorative study, Monrose et al. (2017) asked people why they passed on information they had received at a community health fair. Nearly half of the participants (n = 27 of 60) shared information on cancer screening by giving out brochures from the health fair or telling other people about the information. Reasons for sharing referred to the habitual practice and the perceived value of the information on cancer screening for other people. Huisman and colleagues’ qualitative study (2020) revealed that people may share information to give advice to others. In line with that, informing other people by passing on information from other sources can also be discussed in the tradition of opinion leadership (Fu et al., 2017). Opinion leaders are defined as people who are active media users and who collect, interpret and diffuse media messages to other (less active) media users (Katz & Lazarsfeld, 1955). People who perceive themselves as opinion leaders regarding health topics may share information with others to fulfil this role (MacEachern et al., 2020).
Despite first insights on single reasons, there is a lack of comprehensive data about people’s reasons for information sharing. Moreover, there is also a research gap regarding reasons for not sharing information (Huisman et al., 2020). Hence, we aim to address the following research question:
Research Question 2: What are women’s reasons to share or not share information on mammography screening?
Determinants of health information sharing
To guide our examination of determinants of health information sharing, an established model to explain health information behaviour, including cancer-related information behaviour (e.g., Lewis & Martinez, 2014), will provide the starting point. We choose the theory of motivated information management (Afifi & Weiner, 2004), which is rooted in the uncertainty literature and has mostly been used to examine information seeking (see the review of Kuang & Wilson, 2021). At the same time, it is a model originally focused on interpersonal communication (e.g., Afifi & Weiner, 2006; Fowler & Afifi, 2011). As information sharing comprises a type of information behaviour relying on interpersonal communication, basic assumptions of the theory of motivated information management may also be useful to explain information sharing.
According to the theory of motivated information management, direct cognitive predictors of information behaviour are people’s outcome expectancies and efficacy assessments. Outcome expectancies refer to people’s assessment of the outcome- and process-related benefits and costs of information behaviour. Efficacy assessments describe people’s perceived ability to enact information behaviours (Afifi & Weiner, 2004). For outcome expectancies, there is a lack of research in the context of information sharing. However, it seems plausible that—similarly to other information behaviours such as information seeking—people may also evaluate the potential benefits and costs of information sharing before deciding to do so or not. Regarding efficacy assessments, existing research based on comparable constructs provides some valuable insights. In a study by Yang and Zhuang (2020), people’s perceived information gathering capacity, i.e., their perceived efficacy in performing the information behaviour, did not only predict information seeking but even more so information sharing. However, in a series of surveys, Yang et al. (2022) could only partially confirm this relation. Hence, we argue to consider specific sharing efficacy beliefs in addition to general efficacy assessments mostly referring to seeking behaviours. As a prerequisite of motivated information management, Afifi et al. (2006) also examine issue importance. In line with that, Crook et al. (2016) showed a positive relation between health information sharing and people’s positive appraisal of engaging with issue-related information. In addition to predictors postulated by the theory of motivated information management, Yang et al. (2022) reveal a positive relationship between information sharing and current topic-knowledge. Moreover, previous research points to self-perceived opinion leadership as a specific predictor of information sharing (Bobkowski, 2015; Fu et al., 2017).
Beyond these socio-cognitive factors, previous studies found a significant correlation between information sharing and two types of information retrieval, namely information seeking and/or information scanning (Hayashi et al., 2020; Hong et al., 2021; M. Liu et al., 2019). Regarding sociodemographics, Yang et al. (2022) and Hayashi et al. (2020) showed an impact of individuals’ age and education. Because some of these results are rather preliminary and it remains unclear how far they can be transferred to health information sharing on mammography screening, we derived the following research question:
Research Question 3: How do the theoretically derived socio-cognitive factors, information retrieval and sociodemographics influence information sharing?
Method
Design
To capture actual sharing behaviour of women who have to decide on participating in mammography screening, we conducted a two-wave online survey. In the first survey, participants saw the official invitation letter to mammography screening and were asked to put themselves into the presented situation. Similarly to Fowler et al. (2018), we collected data on behavioural determinants (socio-cognitive factors, sociodemographics) at wave 1 and reported behaviour (information retrieval i.e., information seeking and scanning, and information sharing) at wave 2. After 14 days, the participants were asked about their recent information behaviour and the reasons for (not) sharing information.
Participants
Participants were recruited through an online panel provider. The analysis was limited to the respondents who completed both surveys (n = 1,136 out of 1,400). The sample was stratified to include roughly equal numbers of women who had not yet received an invitation due to age (40-49 years) or who had already been invited (50-69 years), resulting in a mean age of M = 52.57 years (SD = 8.86). We decided to include both groups because experience with the biannual invitation may impact mammography-related information behaviour. Moreover, there is a debate about lowering the age cut-off of the screening programme. Regarding education, the quota sample aimed at a distribution equal to a representative sample of German women. In both the initial sample and the sub-sample of women who took part in both studies, 43% had a secondary school leaving certificate, and a share of 41% had achieved at least high school graduation. The study protocol was approved by the Joint Ethics Committee of Leibniz University Hannover and the Hanover University of Music, Drama, and Media. Informed consent was obtained within the online survey.
Measures
The theoretically derived socio-cognitive factors were measured with established scales. More information on items and scales can be found in the appendix, Table A1.
Outcome expectancies were examined globally regarding different potential forms of engaging with information on mammography screening (seeking, scanning and sharing). The traditional statements about the positive and negative consequences (Fowler & Afifi, 2011; Fowler et al., 2018) were supplemented by goals of information behaviours adopted from the goals associated with health information seeking instrument (Chasiotis et al., 2020). The scale of ten items showed high internal consistency (α = .87, M = 3.50, SD = 1.06).
Efficacy assessments were measured for information seeking and for information sharing. Seeking efficacy (α = .87, M = 4.18, SD = .80) was captured using four items adapted from the perceived behavioural control measure (Kahlor et al., 2019). For sharing efficacy (α = .87, M = 3.87, SD = 1.02) we adapted a scale from Park et al. (2015) and also measured it with four items.
Issue importance was captured as the importance of engaging with the topic of mammography screening with one item in the style of Fowler et al. (2018) and revealed a high issue importance (M = 4.26, SD = 1.13).
Current topic knowledge was captured in line with Kahlor (2010) by rating the current knowledge of mammography screening on a scale from 0 to 100 (M = 74.02, SD = 24.23).
Opinion leadership was measured as self-designated opinion leadership by adapting the scale of Childers (1986) to the health context. The six items provided high internal consistency (α = .88, M = 3.04, SD = .81).
Information retrieval was captured at wave two to assess the information behaviour between both survey waves. To capture information seeking and scanning, 15 sources were distinguished (see Appendix, Table A2). Because the variance in the frequency of information retrieval was very low, we dichotomized and summarized them and only distinguished whether or not women used mass media like newspapers or television shows (M = .16, SD = .37), one-sided online media such as search engines and websites (M = .21, SD = .41), interactive online media such as online communities and social media (M = .15, SD = .35), or talked to formal and informal interpersonal sources (M = .22, SD = .42).
Information sharing was also measured at wave two asking for its frequency. To comprise different possibilities of information sharing, the question (including a short introduction) read as follows:
Sometimes you may feel the urge to pass on information to other people. In our case, it could be that you wanted to share the information about mammography screening from the first survey, your already existing knowledge, or new information you acquired while seeking for information on mammography screening.
Please think about the time since the first survey. During this period—how often did you share information about mammography screening with others?
All respondents who stated that they had shared information on mammography screening at least once during the past two weeks (n = 239), were asked how often they had shared information with ten different formal and informal interpersonal contacts (see Table 1). Response options were ‘never’, ‘less than once a week’, ‘once a week’, ‘several times a week’, ‘daily’, and ‘several times daily’. Due to low variance in the frequency of information sharing, we dichotomized the variables and just distinguished between “did not share information” (= “never”) and “shared information” regardless of the frequency. In addition, the survey included an open-ended question in order to assess the reasons for sharing or not sharing information—sharers were asked why they shared and non-sharers were asked why they did not share any information on mammography screening. Only two of the sharers did not provide any answer in the open text field. Of the non-sharers, 17 did not answer the open question and nine indicated that they didn’t know why they did not share any information.
Data analysis
To answer RQ1, we examined descriptive results regarding information sharing with different recipients. To examine women’s reasons to share or not share information (RQ2), we analysed the open answers by means of inductive category building (Kuckartz & Rädiker, 2019) supported by MAXQDA 2020. A hierarchical, stepwise (backward likelihood ratio), logistic regression analysis (Field, 2013) was conducted using IBM’s SPSS® 28 to examine the predictors’ influence on information sharing (yes/no) (RQ3).
Results
Extent and recipients of health information sharing (RQ1)
About one fifth of the surveyed women (n = 239 of 1,136) shared information about mammography screening with others in between the two waves. Mostly, they shared with friends, family members and partners (see Table 1). They only rarely shared information with health professionals or weak ties such as work colleagues or neighbours. Very few women shared information with other people through online platforms or social media.
| Recipients | n | % |
|---|---|---|
| Friends | 147 | 12.9 |
| Other family members | 107 | 9.4 |
| Partners | 101 | 8.9 |
| Acquaintances | 94 | 8.3 |
| Health professionals | 65 | 5.7 |
| Work colleagues | 63 | 5.5 |
| Parents | 56 | 4.9 |
| Neighbours | 37 | 3.3 |
| Online-platform users | 32 | 2.8 |
| Social media users | 30 | 2.6 |
Table 1. Frequency of information sharing with different recipients
Reasons for health information sharing (RQ2)
The reasons women gave for sharing information on mammography screening could be empirically distinguished into cause and purpose (see Table 2 for examples of all inductive categories). External causes for information sharing mainly comprised timeliness of the topic (e.g., an appointment for mammography screening), the topic arising from the conversation and inquiries from other people or media coverage on mammography screening. In addition to these external causes, women shared information because of the perceived importance of the topic, personal involvement and communicational as well as informational needs. Exchange of experiences and opinions as well as the desire to educate or convince others were mentioned as most important purposes of sharing.
| Category | Sub-category (Number of codings) | Example |
|---|---|---|
| Cause (external) | Timeliness (46) | ‘Because I got an invitation to the screening.’ |
| Arising from conversation (31) | ‘We came across the topic by chance.’ | |
| Reactivity of survey (11) | ‘Because it was present to me through the questioning.’ | |
| Inquiry (8) | ‘Because I was asked.’ | |
| Occupational (5) | ‘I work in mammography.’ | |
| Media coverage (1) | ‘I saw something on TV about breast cancer.’ | |
| Cause (internal) | Importance of the topic (34) | ‘Because I think the topic is very important.’ |
| Personal involvement (26) | ‘Because a friend has breast cancer.’ | |
| Communication needs (25) | ‘I wanted to know more about how others think about it.’ | |
| Information needs (14) | ‘I am very interested in the topic.’ | |
| Affective reactions (4) | ‘Because of concern.’ | |
| Purpose | Exchange of experiences (23) | ‘Because I was asked about my experience with it.’ |
| Inform and educate others (11) | ‘I wanted to inform a friend.’ | |
| Exchange of opinions (8) | ‘Because I wanted to know other opinions.’ | |
| Raise awareness/convince others (6) | ‘To make the others aware of the subject.’ | |
| Scheduling (4) | ‘Had a screening appointment and informed family members that I would be home later because of it.’ | |
| Emotional support (1) | ‘I told my mother because she had a mammogram coming up and she was very nervous about it. I was able to calm her down a bit.’ |
Note. Sub-categories within one category are sorted by
descending frequency. Answers could be coded with more than one
category. n = 237 (sharers who provided answers to the
open-ended question).
Table 2. Reasons for sharing information
Relations between cause and purpose revealed two dominant facets of information sharing. The cause ‘importance of the topic’ was often mentioned together with the purpose ‘educating others’, e.g., ‘As a 66-year-old woman, it is important for me to give others information about my experiences with mammography screening’.
In contrast to this rather one-sided notion of information sharing, the cause ‘communication need’ was often coded together with the purposes ‘exchange of experiences’ and ‘exchange of opinions’, revealing a more reciprocal perception of information sharing, e.g., ‘To find out what others think about it or to hear their experiences with it’.
Reasons for not sharing any information on mammography screening partially mirrored the respective reasons for sharing (see Table 3). Women stated that they did not share any information because there was no external cause, i.e., the topic did not arise in any conversations, there was no timeliness of the topic, they did not retrieve any new information, or did not receive any inquiries. In addition, participants also mentioned the lack of adequate communication partners. Internal causes, or rather the lack thereof, also mirrored reasons for sharing: Participants explained that they did not share any information because they perceived no need for communication or information or were not personally involved with the topic. In addition to these external and internal causes, respondents referred to topic-specific reasons for not sharing. They did not share any information because other topics were more important, they had no interest in the topic, mammography screening is an intimate topic, or they hold a negative or ambivalent attitude towards mammography screening.
| Category | Sub-category (Number of codings) | Example |
|---|---|---|
| No cause (external) | No arising from conversation (201) | ‘It did not come up.’ |
| No timeliness (73) | ‘It was not an issue for me nor my environment.’ | |
| *No adequate communication partners (72) | ‘I have no one to share it with.’ | |
| No media coverage/new information (15) | ‘I did not come across any information.’ | |
| No inquiry (12) | ‘No one asked me about it.’ | |
| No cause (internal) | No communication/information needs (150) | ‘There was no need to.’ |
| No personal involvement (100) | ‘I have not been actively involved with it, so I have not shared any information about it.’ | |
| *No resources/time (66) | ‘No time for it.’ | |
| *No sharing in general (13) | ‘I never share information with others.’ | |
| Affective reactions (6) | ‘The subject scares me.’ | |
| *Topic-specific | *Higher importance of other topics (99) | ‘I had other problems/worries.’ |
| No interest in topic (70) | ‘The subject does not interest me.’ | |
| *Intimate nature of topic (19) | ‘Because it is too personal.’ | |
| *Negative/ambivalent attitude (15) | ‘I would not do the screening myself.’ | |
| Note. Sub-categories are sorted by descending frequency. *specific reasons for not sharing that do not mirror reasons for sharing. Answers could be coded with more than one category. n = 871 (non-sharers who provided answers to the open-ended question other than ‘don’t know’). | ||
Table 3. Reasons for not sharing information
Determinants of health information sharing (RQ3)
Regarding the determinants of health information sharing addressed in the third research question, bivariate correlations showed that all socio-cognitive and information retrieval factors were significantly related to information sharing (see Appendix, Table A3). The results of the stepwise logistic regression indicated that the determinants explained more than one-third of the variance in information sharing (Nagelkerke's R² = .383). The last step of the final model revealed interpersonal communication (OR = 5.61, p < .001), information retrieval via mass media (OR = 1.93, p = .014) and interactive online communication (OR = 1.79, p = .030) as well as self-designated opinion leadership (OR = 1.64, p < .001) as those most strongly related to information sharing (see Table 4). Moreover, issue importance was positively related to information sharing (OR = 1.29, p = .034). Outcome expectancies remained in the equation but were not significantly related to information sharing (OR = 1.22, p = .069). According to the likelihood ratio criterium, age, education, current knowledge, communication and sharing efficacy, and one-sided online communication were excluded from the equation (see Appendix, Table A4).
| B | SE | Wald | df | p | Exp(B) | |
|---|---|---|---|---|---|---|
| Constant | -5.641 | .607 | 86.329 | 1 | <.001 | .004 |
| Issue importance | .257 | .122 | 4.475 | 1 | .034 | 1.293 |
| Outcome expectancies | .199 | .109 | 3.304 | 1 | .069 | 1.220 |
| Opinion leadership | .495 | .120 | 17.034 | 1 | <.001 | 1.640 |
| Information retrieval via mass media | .657 | .268 | 6.030 | 1 | .014 | 1.930 |
| Interactive online communication | .581 | .267 | 4.726 | 1 | .030 | 1.788 |
| Interpersonal communication | 1.725 | .225 | 58.866 | 1 | <.001 | 5.612 |
Note. n = 1,134. Stepwise backward by likelihood
ratio. The last step of the last block is shown. Nagelkerke's
R² = .383. model Χ2(6) = 318.65, p <
.001. Variables not in the equation: age, education, current knowledge,
communication and sharing efficacy, one-sided online communication.
Table 4. Logistic regression of determinants of
information sharing
Discussion
As most health information behaviour studies are limited to information seeking and scanning (Huisman et al., 2020) or limited to online sharing behaviours (e.g., Huesch et al., 2017; Rosenkrantz et al., 2016), the present study aims to clarify the concept of information sharing by shedding light on its recipients, reasons and determinants. In that, we contribute to the conceptual clarification of health information sharing and suggest a conceptual framework (see Figure 1) depicting the nature of health information sharing and its key determinants to provide guidance for further research.
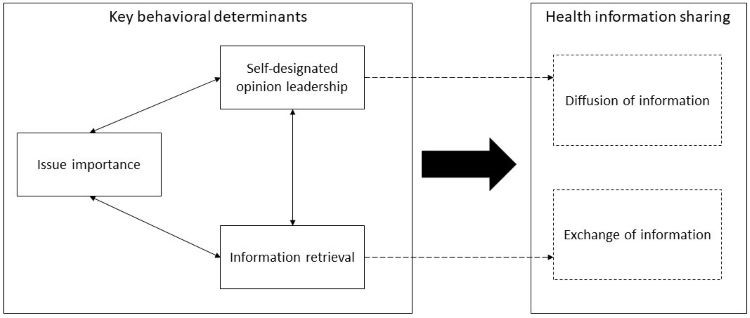
Figure 1. Framework for the concept of health information sharing and its key determinants
After (hypothetically) receiving an invitation to mammography screening, one-fifth of the respondents in our longitudinal study shared information with other people—mainly friends, family members and partners. The fact that respondents mainly shared information with strong ties underlines that information sharing may be a means to maintaining relationships (Southwell, 2017).
Having a closer look at reasons for sharing health information, women’s open answers could be divided into causes and purposes and revealed two different facets of information sharing crucial for conceptual clarity (see Figure 1). On the one hand, information sharing can be understood as the passing on of health-related information. Those women shared information to educate others on a topic perceived as highly important. This aspect of information sharing can be referred to the diffusion of information and the concept of opinion leadership. Opinion leaders fulfil a relay function, reduce complexity, give orientation and arouse interest (Stehr et al., 2015). Accordingly, women’s purposes of information sharing on mammography screening comprised passing on information and educating others, giving orientation regarding the decision about mammography and raising awareness for this important topic. On the other hand, women also shared information because they had informational and communicational needs and wanted to exchange opinions and experiences on mammography screening. This rather reciprocal aspect of information sharing highlights the importance of interpersonal communication as a part of people’s health information behaviour to enable an informed decision about cancer screening (e.g., Nguyen et al., 2010).
These two different aspects of health information sharing can be compared to broader concepts of information sharing in other research fields. In library and information science, researchers also discuss two different perspectives on information sharing (Pilerot, 2012; Savolainen, 2017). The transmission view describes the diffusion of information and focuses on how information is transported from whom to whom. This is similar to the traditional relay function of opinion leaders and a rather unidirectional view of information sharing. In contrast, the ritual view defines information sharing as a mutual or reciprocal exchange of information. In our study, this refers to the exchange of opinions and experiences on mammography screening to make an informed decision. Hence, our research highlights that, also for health information sharing, we must consider both perspectives.
Those are also mirrored in the key determinants of health information sharing we found in our study (see Figure 1). Issue importance was confirmed as a prerequisite of any information behaviour (Afifi et al., 2006). In addition, different forms of information retrieval (mainly interpersonal sources, but also interactive online media and mass media) were strongly related to information sharing. This underlines that different health information behaviour may overlap or lead to each other (Huisman et al., 2020) and discussing what one learned from seeking and scanning information is part of the reflective integration of this information (Lee et al., 2016). Efficacy assessments and outcome expectancies, i.e., the direct predictors of information behaviour according to the theory of motivated information management (Afifi & Weiner, 2004), also correlated with information sharing but were no significant predictors in the regression model. Hence, it remains an open question how far existing information behaviour models are suitable for explaining information sharing. In our study, efficacy assessments and outcome expectancies both correlated with self-designated opinion leadership, which resulted to be strongly related to information sharing behaviour. This is in line with previous studies that understand opinion leaders as gatekeepers in the process of information diffusion (Bobkowski, 2015; MacEachern et al., 2020). As our explorative study showed that the behavioural determinants were intercorrelated, future studies are needed that also consider possible mediation and moderation relations between the different determinants.
Also, the role of emotions should be further explored. While in our study, affective reactions and emotional support were only rarely mentioned as reasons for (not) sharing information in the specific context we created, other studies point out their relevance for health information sharing (Rauscher & Hesse, 2014; Rui, 2023). The minor role of emotions in our specific context could be due to the hypothetical situation which may induce fewer emotions than a real-life situation. Moreover, the inductive analysis of the open-ended questions on (not) sharing information revealed that, in addition to planned information sharing, sharing may also occur spontaneously (Huisman et al., 2020). Women shared information on mammography screening because it arose from the conversation; other women stated that they did not share any information because the topic did not arise, and they had no adequate conversation partners. In accordance with this result, previous studies have demonstrated that people tend to share more information if they have spaces and interaction partners to do so (Southwell, 2017). This could also explain why only one respondent mentioned sharing information to provide emotional support. Social support is something respondents would have provided for someone currently in need. Similarly to information sharing in general this requires an external cause like timeliness or the issue arising from the conversation. It is plausible that only a few respondents found themselves in such circumstances during the timespan of two weeks. Future studies must examine how these situational factors can be integrated into explaining health information behaviour, especially information sharing. In line with that, future studies should not only investigate predictors on an individual level but also consider network characteristics such as people’s centrality in a community or their intermediary role (Southwell, 2017).
A key strength of our study is that we did not measure behavioural intentions but actual sharing behaviour. However, we only created a hypothetical situation as an inducement of health information behaviour. This limits the external validity of our data. Although information behaviour on cancer in general and mammography screening in particular occurs rather rarely (Kelly et al., 2010; Shim et al., 2006), the low frequency of information sharing could also be explained by the hypothetical situation we created. Hence we cannot make any statements about the prevalence of information sharing in a real-world setting. Moreover, in our study, there was only low variance in the frequency of information behaviour between the two survey waves. This could be due to the retrospective survey design. Future studies could implement experience sampling methods (Schnauber-Stockmann & Karnowski, 2020) to capture the information behaviour in situ. This would also provide the opportunity to integrate the situational factors leading to unplanned information sharing into the design. Moreover, future studies could also consider what kind of information people share for what facets of information sharing. Answers to the open-ended questions in our survey were rather short and did not allow for any in-depth analysis. Further qualitative studies are needed to shed light on the meaning of different causes and purposes of information sharing.
Conclusion
Information sharing is an important but under researched type of health information behaviour. Our study examined characteristics, reasons and determinants of information sharing and revealed two facets of this concept: information sharing in the sense of selecting and passing on information (cf. diffusion of information by opinion leaders), and information sharing as the mutual exchange of opinions and experiences. Both facets should be considered to comprehensively examine health information sharing behaviours and their relation with informed decision making.
Practice implications
Referring to the two facets of information sharing (diffusion and exchange of information), some practical implications for health communication and healthcare can be derived. For both aspects, the perceived issue importance is a key prerequisite of information sharing. Hence, communication on, e.g., mammography screening, should stress its relevance for people’s lives. To ensure diffusion of information to less interested or involved people, a promising strategy may be to identify opinion leaders within a community and support them in sharing information with their family and friends. Our study confirmed that interpersonal communication on health issues like mammography screening is an important part of dealing with obtained information and reaching an informed decision. Therefore, the reciprocal exchange of information and experiences amongst peers should be cultivated.
Acknowledgements
The authors would like to thank the anonymous reviewers for their valuable feedback.
About the authors
Paula Stehr (Ph.D., University of Erfurt) is a postdoctoral researcher at the Department of Media and Communication, LMU Munich, Germany. She is currently working as a guest professor at the University of Augsburg. Her research focuses on health communication and digital media, comprising topics such as evidence-based health campaigns and health information behaviour. She can be contacted at paula.stehr@lmu.de
Elena Link (Ph.D., Hanover University of Music, Drama and Media) is an Assistant Professor at the Department of Communication at the Johannes Gutenberg University of Mainz, Germany. In her research, she studies health and risk information-seeking and avoidance behaviours, their influencing factors, and outcomes. She can be contacted at elena.link@uni-mainz.de
Constanze Rossmann (Ph.D., LMU Munich) is a full professor for communication science at the Department of Media and Communication, LMU Munich. Her research focuses on health communication, specifically evidence-based campaign development, digital media in health communication, and crisis communication. She is co-founder of the Health Communication Division within the German Communication Association (DGPuK). She can be contacted at constanze.rossmann@lmu.de
References
Abelson, J., Tripp, L., & Sussman, J. (2018). ‘I just want to be able to make a choice’: results from citizen deliberations about mammography screening in Ontario, Canada. Health Policy, 122(12), 1364–1371. https://doi.org/10.1016/j.healthpol.2018.09.013
Afifi, W. A., Morgan, S. E., Stephenson, M. T., Morse, C., Harrison, T., Reichert, T., & Long, S. D. (2006). Examining the decision to talk with family about organ donation: applying the theory of motivated information management. Communication Monographs, 73(2), 188–215. https://doi.org/10.1080/03637750600690700
Afifi, W. A., & Weiner, J. L. (2004). Toward a theory of motivated information management. Communication Theory, 14(2), 167–190. https://doi.org/10.1093/ct/14.2.167
Afifi, W. A., & Weiner, J. L. (2006). Seeking information about sexual health: applying the theory of motivated information management. Human Communication Research, 32(1), 35–57. https://doi.org/10.1111/j.1468-2958.2006.00002.x
Ashida, S., & Schafer, E. J. (2015). Family health information sharing among older adults: reaching more family members. Journal of Community Genetics, 6(1), 17–27. https://doi.org/10.1007/s12687-014-0197-x
Binda, J., Yuan, C. W., Cope, N., Park, H., Choe, E. K., & Carroll, J. M. (2018). Supporting effective sharing of health information among intergenerational family members. In N. Minsky (Ed.), ACM Other conferences, Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare (pp. 148–157). ACM. https://doi.org/10.1145/3240925.3240936
Bobkowski, P. S. (2015). Sharing the news: effects of informational utility and opinion leadership on online news sharing. Journalism & Mass Communication Quarterly, 92(2), 320–345. https://doi.org/10.1177/1077699015573194
Chasiotis, A., Wedderhoff, O., Rosman, T., & Mayer, A.‑K. (2020). Why do we want health information? The goals associated with health information seeking (GAINS) questionnaire. Psychology & Health, 35(3), 255–274. https://doi.org/10.1080/08870446.2019.1644336
Childers, T. L. (1986). Assessment of the psychometric properties of an opinion leadership scale. Journal of Marketing Research, 23(2), 184. https://doi.org/10.2307/3151666
Crook, B., Stephens, K. K., Pastorek, A. E., Mackert, M., & Donovan, E. E. (2016). Sharing health information and influencing behavioral intentions: the role of health literacy, information overload, and the internet in the diffusion of healthy heart information. Health Communication, 31(1), 60–71. https://doi.org/10.1080/10410236.2014.936336
Döbrössy, B., Girasek, E., Susánszky, A., Koncz, Z., Győrffy, Z., & Bognár, V. K. (2020). “Clicks, likes, shares and comments” a systematic review of breast cancer screening discourse in social media. PloS One, 15(4), e0231422. https://doi.org/10.1371/journal.pone.0231422
Field, A. (2013). Discovering statistics using IBM SPSS statistics: and sex and drugs and rock ‘n’ roll (4th ed.). Sage.
Fowler, C., & Afifi, W. A. (2011). Applying the theory of motivated information management to adult children’s discussions of caregiving with aging parents. Journal of Social and Personal Relationships, 28(4), 507–535. https://doi.org/10.1177/0265407510384896
Fowler, C., Gasiorek, J., & Afifi, W. A. (2018). Complex considerations in couples’ financial information management: Extending the theory of motivated information management. Communication Research, 45(3), 365–393. https://doi.org/10.1177/0093650216644024
Fu, H., Dong, D., Da Feng, He, Z., Tang, S., Fu, Q., & Feng, Z. (2017). To share or not to share: a cross-sectional study on health information sharing and its determinants among Chinese rural chronic patients. Journal of Health Communication, 22(10), 800–807. https://doi.org/10.1080/10810730.2017.1360414
Hayashi, H., Tan, A. S. L., Kawachi, I., Ishikawa, Y., Kondo, K., Kondo, N., Tsuboya, T., & Viswanath, K. (2020). Interpersonal diffusion of health information: health information mavenism among people age 65 and over in Japan. Health Communication, 35(7), 804–814. https://doi.org/10.1080/10410236.2019.1593078
Heinig, M., Schäfer, W., Langner, I., Zeeb, H., & Haug, U. (2023). German mammography screening program: Adherence, characteristics of (non-)participants and utilization of non-screening mammography-a longitudinal analysis. BMC Public Health, 23(1), 1678. https://doi.org/10.1186/s12889-023-16589-5
Hong, Y., Wan, M., & Li, Z. (2021). Understanding the health information sharing behavior of social media users. Journal of Organizational and End User Computing, 33(5), 180–203. https://doi.org/10.4018/JOEUC.20210901.oa9
Hornik, R., Parvanta, S., Mello, S., Freres, D., Kelly, B., & Schwartz, J. S. (2013). Effects of scanning (routine health information exposure) on cancer screening and prevention behaviors in the general population. Journal of Health Communication, 18(12), 1422–1435. https://doi.org/10.1080/10810730.2013.798381
Huesch, M., Chetlen, A., Segel, J., & Schetter, S. (2017). Frequencies of private mentions and sharing of mammography and breast cancer terms on Facebook: a pilot study. Journal of Medical Internet Research, 19(6), e201. https://doi.org/10.2196/jmir.7508
Huisman, M., Biltereyst, D., & Joye, S. (2020). Sharing is caring: The everyday informal exchange of health information among adults aged fifty and over. Information Research: An International Electronic Journal, 25(1). (Archived by the Internet Archive at https://web.archive.org/web/20200224193450/http://informationr.net/ir/25-1/paper848.html)
Kahlor, L. (2010). Prism: A planned risk information seeking model. Health Communication, 25(4), 345–356. https://doi.org/10.1080/10410231003775172
Kahlor, L., Wang, W., Olson, H. C., Li, X., & Markman, A. B. (2019). Public perceptions and information seeking intentions related to seismicity in five Texas communities. International Journal of Disaster Risk Reduction, 37, 101147. https://doi.org/10.1016/j.ijdrr.2019.101147
Katz, E., & Lazarsfeld, P. F. (1955). Personal influence: The part played by people in the flow of mass communications. Foundations of communications research: Vol. 2. Free Press.
Keating, N. L., & Pace, L. E. (2018). Breast cancer screening in 2018: Time for shared decision making. JAMA, 319(17), 1814–1815. https://doi.org/10.1001/jama.2018.3388
Kelly, B., Hornik, R., Romantan, A., Schwartz, J. S., Armstrong, K., DeMichele, A., Fishbein, M., Gray, S., Hull, S., Kim, A., Nagler, R., Niederdeppe, J., Ramírez, A. S., Smith-McLallen, A., & Wong, N. (2010). Cancer information scanning and seeking in the general population. Journal of Health Communication, 15(7), 734–753. https://doi.org/10.1080/10810730.2010.514029
Kuang, K., & Wilson, S. R. (2021). Theory of motivated information management: A meta-analytic review. Communication Theory, 31(3), 463–490. https://doi.org/10.1093/ct/qtz025
Kuckartz, U., & Rädiker, S. (2019). Analyzing qualitative data with MAXQDA: Text, audio, and video. Springer eBooks Social Sciences. Springer.
Lee, C.‑J., Zhao, X., & Pena-y-Lillo, M. (2016). Theorizing the pathways from seeking and scanning to mammography screening. Health Communication, 31(1), 117–128. https://doi.org/10.1080/10410236.2014.942769
Lewis, N., & Martinez, L. S. (2014). Does the number of cancer patients’ close social ties affect cancer-related information seeking through communication efficacy? Testing a mediation model. Journal of Health Communication, 19(9), 1076–1097. https://doi.org/10.1080/10810730.2013.872724
Liu, J., King, A. J., Margolin, D., & Niederdeppe, J. (2020). Information seeking and scanning about colorectal cancer screening among black and white americans, ages 45-74: Comparing information sources and screening behaviors. Journal of Health Communication, 25(5), 402–411. https://doi.org/10.1080/10810730.2020.1776424
Liu, M., Yang, Y., & Sun, Y. (2019). Exploring health information sharing behavior among Chinese older adults: A social support perspective. Health Communication, 34(14), 1824–1832. https://doi.org/10.1080/10410236.2018.1536950
MacEachern, L., Cranley, L., Curran, J., & Keefe, J. (2020). The role of motivation in the diffusion of innovations in Canada’s long-term care sector: A qualitative study. Implementation Science Communications, 1(1), 79. https://doi.org/10.1186/s43058-020-00069-7
Monrose, E., Ledergerber, J., Acheampong, D., & Jandorf, L. (2017). Cancer screening information at community health fairs: What the participants do with information they receive. Journal of Public Health Research, 6(2), 866. https://doi.org/10.4081/jphr.2017.866
Naeem, I., Quan, H., Singh, S., Chowdhury, N., Chowdhury, M., Saini, V., & Tc, T. (2022). Factors associated with willingness to share health information: Rapid review. JMIR Human Factors, 9(1), e20702. https://doi.org/10.2196/20702
Nguyen, G. T., Shungu, N. P., Niederdeppe, J., Barg, F. K., Holmes, J. H., Armstrong, K., & Hornik, R. C. (2010). Cancer-related information seeking and scanning behavior of older Vietnamese immigrants. Journal of Health Communication, 15(7), 754–768. https://doi.org/10.1080/10810730.2010.514034
Park, N., Oh, H. S., & Kang, N. (2015). Effects of ego involvement and social norms on individuals’ uploading intention on Wikipedia: A comparative study between the United States and South Korea. Journal of the Association for Information Science and Technology, 66(7), 1494–1506. https://doi.org/10.1002/asi.23262
Pilerot, O. (2012). Lis research on information sharing activities – people, places, or information. Journal of Documentation, 68(4), 559–581. https://doi.org/10.1108/00220411211239110
Rauscher, E. A., & Hesse, C. (2014). Investigating uncertainty and emotions in conversations about family health history: A test of the theory of motivated information management. Journal of Health Communication, 19(8), 939–954. https://doi.org/10.1080/10810730.2013.837558
Rosenkrantz, A. B., Labib, A., Pysarenko, K., & Prabhu, V. (2016). What do patients tweet about their mammography experience? Academic Radiology, 23(11), 1367–1371. https://doi.org/10.1016/j.acra.2016.07.012
Rui, J. R. (2023). Health information sharing via social network sites (SNSs): Integrating social support and socioemotional selectivity theory. Health Communication, 38(11), 2430–2440. https://doi.org/10.1080/10410236.2022.2074779
Savolainen, R. (2017). Information sharing and knowledge sharing as communicative activities. Information Research: An International Electronic Journal, 22(3), Article Paper 767. http://www.informationr.net/ir/22-3/paper767.html (Archived by WebCite® at http://www.webcitation.org/6tTRz0IcS)
Schnauber-Stockmann, A., & Karnowski, V. (2020). Mobile devices as tools for media and communication research: A scoping review on collecting self-report data in repeated measurement designs. Communication Methods and Measures, 14(3), 145–164. https://doi.org/10.1080/19312458.2020.1784402
Shim, M., Kelly, B., & Hornik, R. (2006). Cancer information scanning and seeking behavior is associated with knowledge, lifestyle choices, and screening. Journal of Health Communication, 11 Suppl 1, 157–172. https://doi.org/10.1080/10810730600637475
Shneyderman, Y., Rutten, L. J. F., Arheart, K. L., Byrne, M. M., Kornfeld, J., & Schwartz, S. J. (2016). Health information seeking and cancer screening adherence rates. Journal of Cancer Education: The Official Journal of the American Association for Cancer Education, 31(1), 75–83. https://doi.org/10.1007/s13187-015-0791-6
Southwell, B. G. (2017). Promoting popular understanding of science and health through social networks. In K. H. Jamieson, D. M. Kahan, D. A. Scheufele, & B. G. Southwell (Eds.), The Oxford handbook on the science of science communication (pp. 223–231). Oxford University Press.
Southwell, B. G., Slater, J. S., Nelson, C. L., & Rothman, A. J. (2012). Does it pay to pay people to share information? Using financial incentives to promote peer referral for mammography among the underinsured. American Journal of Health Promotion: AJHP, 26(6), 348–351. https://doi.org/10.4278/ajhp.110120-ARB-34
Stehr, P., Rössler, P., Leissner, L., & Schönhardt, F. (2015). Parasocial opinion leadership. Media personalities’ influence within parasocial relations: Theoretical conceptualization and preliminary results. International Journal of Communication, 9, 982–1001. http://ijoc.org/index.php/ijoc/article/view/2717/1350
van Agt, H., Fracheboud, J., van der Steen, A., & Koning, H. de (2012). Do women make an informed choice about participating in breast cancer screening? A survey among women invited for a first mammography screening examination. Patient Education and Counseling, 89(2), 353–359. https://doi.org/10.1016/j.pec.2012.08.003
Yang, J. Z., Liu, Z., & Wong, J. C. S. (2022). Information seeking and information sharing during the COVID-19 pandemic. Communication Quarterly, 70(1), 1–21. https://doi.org/10.1080/01463373.2021.1995772
Yang, J. Z., & Zhuang, J [Jun] (2020). Information seeking and information sharing related to hurricane Harvey. Journalism & Mass Communication Quarterly, 97(4), 1054–1079. https://doi.org/10.1177/1077699019887675
Zhuang, J [Jie], & Guan, M. (2021). Modeling the mediating and moderating roles of risk perceptions, efficacy, desired uncertainty, and worry in information seeking-cancer screening relationship using HINTS 2017 data. Health Communication, 37(7), 897–908. https://doi.org/10.1080/10410236.2021.1876324
Appendix I
| Construct | Example of item wording | Source |
|---|---|---|
| Outcome expectancies: Positive and negative consequences1 | If I dealt with information about mammography screening in the future, this would have more positive than negative effects on the relationships with the people around me. | Fowler et al. (2018); Fowler & Afifi (2011) |
| Outcome expectancies: Goals of information behaviours1 | If I dealt with information about mammography screening in the future, it would help me figure out what I can do to deal with the issue. | adopted from the GAINS instrument (Chasiotis et al., 2020) |
| Efficacy assessments: Seeking efficacy1 | I know how to find information about mammography screening. | Kahlor et al. (2019) |
| Efficacy assessments: Sharing efficacy1 | It is easy for me to share information about mammography screening with others. | Park et al. (2015) |
| Issue importance2 | How important does it seem to you personally to be engaged with the topic of mammography screening? | Fowler et al. (2018) |
| Current topic knowledge | Please rate your current knowledge about the risks and benefits of mammography screening on a scale of 0 to 100. Zero means knowing nothing. 100 means knowing everything you could know about the risks and benefits of mammography. | Kahlor (2010) |
| Opinion leadership3 | Compared to your circle of friends and acquaintances, how likely are you to be asked for your opinion on health topics? | Childers (1986) |
1 measured on a five-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree) 2 measured on a five-point Likert-type scale ranging from 1 (not important at all) to 5 (very important) 3 measured on a five-point Likert-type scale ranging from 1 (very unlikely) to 5 (very likely) |
||
Table A1. Measures of socio-cognitive factors
| Source | Items included |
|---|---|
| Mass media | Information seeking newspapers Information seeking magazines Information seeking TV programmes Information seeking radio and podcasts Information scanning newspapers Information scanning magazines Information scanning TV programmes Information scanning radio and podcasts |
| One-sided online media | Information seeking search engines Information seeking online encyclopaedia Information seeking health-related web portals Information seeking specialist online information Information scanning search engines Information scanning online encyclopaedia Information scanning health-related web portals Information scanning specialist online information |
| Interactive online media | Information seeking social network sites Information seeking online communities Information seeking blogs Information scanning social network sites Information scanning online communities Information scanning blogs |
| Interpersonal sources | Information seeking family members Information seeking friends Information seeking colleagues Information seeking health professionals Information scanning family members Information scanning friends Information scanning colleagues Information scanning health professionals |
| Note. Response options for each item were “never”, “less than once a week”, “once a week”, “several times a week”, “daily”, and “several times daily”. Measures were combined and dichotomized into “did not retrieve information” vs. “did retrieve information” from each of the four sources. Example: Answers were coded as “did retrieve information” from mass media if respondents answered something different from “never” for at least one of the respective items (regardless if information seeking or scanning). | |
Table A2. Measures of information retrieval
| Construct | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Info sharing | – | ||||||||||
| 2. Issue importance | .19** | – | |||||||||
| 3. Outcome expectancies | .20** | .58** | – | ||||||||
| 4. Current knowledge | .08** | .18** | .14** | – | |||||||
| 5. Communication efficacy | .09** | .14** | .16** | .44** | – | ||||||
| 6. Sharing efficacy | .11** | .15** | .21** | .31** | .54** | – | |||||
| 7. Opinion leadership | .25** | .23** | .24** | .19** | .26** | .32** | – | ||||
| 8. Information retrieval mass media | .43** | .15** | .14** | .05** | .06 | .05 | .16** | – | |||
| 9. One-sided online media | .43** | .19** | .21** | .07* | .10** | .07* | .21** | .62** | – | ||
| 10. Interactive online media | .41** | .13** | .13** | .04 | .04 | .05* | .18** | .67** | .69** | – | |
| 11. Interpersonal communication | .51** | .17** | .18** | .10** | .10** | .11** | .24** | .64** | .74** | .61** | – |
Note. n = 1,136, *p < .05. **p < .01
Table A3. Correlations of information sharing with
socio-cognitive determinants and information retrieval
| Score | df | p | ||
|---|---|---|---|---|
| Block 1: Sociodemographics | Age | 2.238 | 1 | .135 |
| High education | .146 | 2 | .930 | |
| Medium education | .144 | 1 | .705 | |
| Low education | .009 | 1 | .925 | |
| Block 2: Sociocognitive factors | Current knowledge | .053 | 1 | .818 |
| Communication efficacy | .151 | 1 | .698 | |
| Sharing efficacy | .087 | 1 | .768 | |
| Block 3: Information retrieval | One-sided online communication | .008 | 1 | .927 |
Note. n = 1,134. Stepwise backward by likelihood ratio. The
last step of the respective block is shown.
Table A4. Logistic regression of determinants of
information sharing—variables not in the equation