vol. 16 no. 3, September, 2011
vol. 16 no. 3, September, 2011 |
||||
With an increase of access to the Internet and free access to numerous types of current awareness services available through the Internet, it seems timely to explore interest in current awareness services from different professional groups. This article focuses on the interest of oncology nurses, specialising in cancer care. Apart from work environments presenting new challenges such as cancer patient education (Echlin and Rees 2002; Hartigan 2003; Hughes et al. 2000; Jenkins 1997; Mahon and Williams 2000; Tarzian, Iwata and Cohen 1999; Thomson 2000; Van der Molen 1999), there is an increase in the number of cancer patients, as well as interest in the use of technology in cancer prevention (Jimbo et al. 2006). The increase in cancer patients was also noted during the study reported in this article: 'Cancer in general has increased a lot in the last year… much more intensive' (All quotations originally in Afrikaans have been translated). According to Dickerson et al. (2006: E16)'nurses should be open to discussion of the information that patients bring to the interaction. Nurses also should be knowledgeable about useful Web sites and online support groups to recommend to patients'.
The purpose of the survey was to explore whether oncology nurses are using current awareness services and if not, whether they would be interested in them, and how such interest can be stimulated. The purpose was not to generalise findings based on the input of a small, purposive, convenience sample, but to explore the refinement of research methods and data collection and new routes (e.g., theories and models of information behaviour) to expand the study and build a model for the use of current awareness services by oncology nurses.
Factors leading to the study are discussed by Fourie and Claasen-Veldsman (2005, 2007a, 2007b) and can be summarised as follows:
The survey attempted to determine the need and interest for current awareness amongst oncology nurses. It is hoped that the findings can promote the use of Internet current awareness services available for free and to refine research methodology to do more extensive local and internationally comparative studies. This might pave the way for studies with other health care professionals, bearing in mind that'oncology is different from anything else…' (All quotations originally in Afrikaans have been translated).
The study focused on a number of influencing factors and interests noted by a mixture of positions (i.e., an oncologist, unit manager, Sister, nurses, staff nurses, etc). This paper reports on:
Oncology is the field of medicine devoted to cancer and the study of tumours (Medicine Net 2003), and oncology nursing concerns cancer patients. Fourie and Claasen-Veldsman (2006: 38) cite a very apt description from Nursing Spectrum which explains an oncology nurse as someone who 'cares for patients with the diagnosis of cancer in various settings; utilizes an emphatic and caring approach to patients whose diagnosis and treatment are often painful and life threatening; administers chemotherapy, conducts patient teaching, and manages illness- and treatment-related symptoms'.
Although there are numerous definitions of current awareness services and alerting services (often used interchangeably with current awareness services), the emphasis is that these are services to help people keep track of current developments and the latest information. Fourie defines current awareness services as:
a selection of one or more systems that provide notification of the existence of new entities added to the system's database or of which the system took note (e.g., documents, web sites, events such as conferences, discussion groups, editions of newsletters). CAS automatically notify users or allow users to check periodically for updates. The entities can be specified according to users' subject interests or according to the type of entity (e.g., books or newsletters) (Fourie 1999: 282).
Many interpretations of information behaviour have also been offered. Widely accepted is the encapsulating definition of Wilson (1999a: 249), explaining information behaviour as'the totality of human behavior in relation to sources and channels of information, including both active and passive information-seeking and information use'. Fisher et al. (2005: xix) define information behaviour as'how people need, seek, give and use information in different contexts'. In the context of this article, information behaviour is interpreted as how people (in this case oncology nurses) need information (including factual information, retrospective searches and information to stay abreast), their interest or lack of interest in information, the sources and channels that they prefer (i.e., how they actually seek the information) and the factors that influence their behaviour to search for information and use it, or not to do this. Although the study focuses on the use of current awareness services (i.e., information monitoring), it also addresses the encapsulating information behaviour of oncology nurses.
An exploratory study based on purposive, convenience sampling was conducted at a medical oncology centre and two oncology hospital wards in Pretoria (South Africa). One of the wards mostly treats patients receiving intensive chemotherapy, stem cell transplants, etc., while the other mostly treats patients who are terminally ill (needing palliative care), as well as children (needing paediatric care). The sample is depicted in Table 1.
| Medical oncology centre | Hospital oncology wards |
|---|---|
| Head oncologist (management) (1) | Ward unit manager (Sister) (1) |
| Oncology nurses (Sisters) (5) | Oncology nurses (Sisters, staff nurses, assistant nurses) (16) |
| Oncology social worker (1) | Care workers (2) |
The medical oncology unit and hospital wards serve the same patients. However, they function under different management, funding and administrative structures (as explained in more detail in sections 7.2.2 and 7.2.3). The study covers the views of management (the head oncologist and the hospital ward unit manager) as well as staff members on different levels (e.g., Sisters, nurses and care workers). Both the medical centre and the hospital wards rely on the support of a multi-disciplinary team including dieticians, physiotherapists and pharmacists. An oncology social worker (a staff member of the medical oncology centre) that consults with centre patients and staff from both the centre and hospital wards was also included.
Although a small survey, it was felt that both groups are sufficiently representative of leading oncology settings in South Africa for exploratory purposes. (Many studies with similar small groups of participants have been reported e.g., studies with twenty patients each by Dickerson et al. (2006) and Andreassen et al. (2005) However, when expanding the survey, participants from academic hospitals and nursing students specialising in oncology nursing should also be included. Permission for the study was obtained from the university's research ethics committee, head oncologist, hospital management and unit manager of the hospital wards.
Due to heavy work schedules and staff shortages, the hospital could not immediately participate. The study with the oncology medical centre was conducted in September 2005, while the study with the hospital wards was conducted in January 2006. The head oncologist suggested participants, while the hospital unit manager called on all staff members available on the two days the researchers visited the wards.
The study is based on a literature survey and empirical study. Apart from the methods used, suggestions for adaptations for further research are offered.
A wide variety of databases in the field of information science, nursing and medicine were searched, namely CINAHL, Library and Information Science Abstracts, Library Literature and Information Science, Social SciSearch, Medline, AIDS and Cancer Research Abstracts, Conference Papers Index, Applied Social Sciences Index and Abstracts, ScienceDirect, Emerald and Web of Science. It showed that very little is known about the information seeking behaviour of oncology nurses. In one of very few studies on the information needs of oncology nurses, Fitch, Chart and Parry (1998) report on their information needs with regard to breast diseases. Most of the nurses felt that they experienced no gap in their knowledge, and therefore did not need information. Cobb and Baird (1999) report on how oncology nurses use the Internet for drug information, literature searches, academic information, patient education, and continuing education. Nothing could be traced on the provision of current awareness services for oncology nurses.
Slightly more is known about the information needs of nurses in general. In an early study, Wakeham (1992) found that nursing students are not readers and that they prefer to consult with colleagues to satisfy information needs. A preference to consult colleagues, reference manuals, textbooks and protocol manuals is also confirmed by Cogdill (2003). According to McCaughan et al. (2005) nurses prefer humanised sources of information including help lines, e-mail discussion groups and networking with colleagues. Their knowledge of CD-ROM and other electronic databases in general was low. Secco et al. (2006) also stress the preference for printed sources such as textbooks and reference works and inter-personal communication, while nurses with higher levels of computer skills used more computer-based sources. Anthony (2000) reports on an international comparison of computer networks' use and potential use in a health care context. Not surprisingly there seem to be significant differences between poor and rich countries with respect to access to networking facilities. There was a significant difference between rich and poor countries with respect to the World Wide Web and USENET, with richer countries having greater access. Anthony (2000) noted enthusiasm for using computer networks in poorer and geographically more remote countries. From a list of ten services available through the Internet, the network resource most valued by nursing organizations was online databases; the least valued was videoconferencing.
In 2003 Estabrooks et al. reported low Internet use at work for nurses, even though there is an increase in its use at home. According to Wozar and Worona (2003:216)'Practicing clinical nurses will use online medical information resources if they are first introduced to them and taught how to access and use them'. In their study, Dee and Stanley (2005) found participants (clinical nurses and nursing students) were very keen on training in database searching if they had better computer skills. Nicholas et al. (2005: 39) and Bertulis and Cheeseborough (2008) noted very poor access to computers and the Internet for nurses.
Nurses require information because of encounters with patients (Cogdill 2003) as well as for decision-making in evidence-based practices (French 1998). Bertulis and Cheeseborough (2008: 187) confirm a patient care focus in the needs of nurses.
Other reports on the information seeking of nurses that are worth noting include Sundin's (2002) report on nurses' information seeking and use as participation in occupational communities, Cogdill's (2003) work on primary care nursing practitioners, Urquhart and Crane's (1994) report on nurses' information-seeking skills and perceptions of information sources, Barta's (1995) report on the information seeking of paediatric nurse educators, Verhey's (1999) discussion of information literacy as part of an undergraduate nursing curriculum and Gregg and Wozar's (2003) report on a training course to help nurses to use Internet health-related sources. In a study by McCaughan et al. (2005) a nurse reported accepting a site with commercial interest as highly reliable on diabetes because of the Website address. (A similar experience was confirmed by one of our participants.) This study also found that nurses were more inclined to use the Internet at home where the presence of family members (expert users) was welcomed.
Practice nurses and nurse practitioners have easier access to computers than other groups of nurses working in the community but require further training in information technology and critical appraisal skills, along with protected time, if they are to exploit the information resources that are becoming increasingly available to them online (McCaughan et al. 2005: 496).
McKnight (2007: 70) reports on the information seeking of on-duty critical care nurses: 'No one can retrieve reliable literature and systematically review it while watching monitors, checking on patients, administering and verifying therapies, and answering telephone calls… They respect research-informed practice and want the best of what academia and libraries can give them to support the care of their patients. However, their duties leave no room for such pursuits… Given the economic realities of health care, hospital administrators are unlikely to pay nurses for off duty time for such pursuits. What they do, they have to do on their own time'. This is in line with the findings by MacIntosh-Murray and Choo (2005: 1332) that'front-line staff are task driven, coping with heavy workloads that limit their attention to and recognition of potential information needs and gaps'.
To put the information-seeking behaviour of oncology and other nurses in context, one should note some of the findings concerning clinicians and other health care workers: Andrews et al. (2005), for example, found that typical barriers for primary care practitioners include lack of time, cost of using resources, the format of information resources and their information seeking skills, while Cullen (2002) found that most family practitioners urgently need training in searching and evaluating information from the Internet. In a study conducted in New Zealand, Cullen (2002) found that most family practitioners did not have access to high quality information sources.
French (2006), exploring uncertainty and information needs in nursing, noted the difficulty in recognising and articulating information needs as well as different types of uncertainty, namely: known or accepted uncertainty, hidden (unaware) uncertainty, unrecognised (ignored) uncertainty and pragmatic uncertainty. Such uncertainty impacts on information seeking.
Although these research reports explain the research methods and data collection, it was interesting to note that they did not dwell on problems experienced. (Boisson and Docsi (2005) is an exception, reporting difficulty in making appointments with female general practitioners, probably because of their busy schedules.) For the reported study it was found that this is one aspect that can have a major impact on further research with oncology nurses. Methods that were reported include a large survey based on questionnaires and interviews (Estabrooks et al. 2003); participant observation and in-context interviews (McKnight 2006); questionnaires, interviews and observation with twenty-five nursing students and twenty-five clinical nurses (Dee and Stanley 2005); questionnaires (300 nursing professionals) and interviews (twenty nursing professionals) (Cogdill 2003); and interviews, observation and documentary analysis with a purposive sample of twenty-nine practice nurses and four nurse practitioners (McCaughan et al. 2005).
The methods for data collection used in the before-mentioned studies (reporting on qualitative and quantitative methods) as well as studies on information-seeking behaviour in general (e.g., as reported by Case 2006; Fourie 2002) were considered in addition to the demanding nature of the work of oncology nurses. The following methods were selected:
Although aware of the hectic schedules of the participants as well as the emotionally demanding nature of their jobs, it was felt that the combination of methods would enable the collection of information-rich data, which was considered essential for purposes of the study. By means of the questionnaire we hoped to collect more detailed information on individual information behaviour .
The (rather detailed) questionnaire was tested with three participants (two from the centre and one from the hospital wards) and adapted; it went through two iterations. [The final version of the questionnaire can be found here].
The survey of staff of the medical oncology centre was completed in September 2005. In addition to the questionnaire, two focus group interviews were conducted with the centre staff. These were followed by an interview with the head oncologist.
Based on the survey with the medical oncology centre, the methods for data collection were adapted. Apart from the expected hectic schedules, they were working with serious staff shortages: it was obvious that they would not have time to complete the questionnaire and that focus group interviews would not be possible. Since they need to take care of patients, complete rounds with doctors and other urgent responsibilities, it is almost impossible to free more than one staff member at a time: 'If you get two of them together at the same time you are lucky'. The questionnaire was used as a guideline for individual interviews, and the questions were adapted according to answers.
The survey with the hospital staff was conducted in January 2006. It started with an individual interview with the unit manager, who holds the rank of Sister. The interview was according to the same schedule as for the head oncologist.
Over two days, interviews were conducted with the staff on duty. Being on site and available for a large part of the day was an effective way to gather data, as it provided a valuable opportunity to speak to the staff and also to glean more perceptions and information from them than would be possible from the questionnaire alone. It was also valuable as it provided an opportunity to explain what was meant by concepts such as current awareness service and the different techniques used. Not only Sisters, but also other staff levels, including the care workers, were included. Although this method of data collection saved much of the participants' time, it meant very intensive interviewing for the researchers.
Both researchers were present during all the interviews. The interviews were tape recorded with the consent of participants, and notes were also taken by one of the researchers. Due to the nature of the project (exploratory) it was not considered necessary to do a verbatim transcription of the interviews.
Questions covered the following:
An interview schedule was used for the interviews with management. It included the following broad categories: task environment, staff information, access provided to information and information communication technology (ICT), expectations for staff to use ICT and information, institution's expectations for staff to use current awareness services, institutional support offered to staff to become aware of new developments, importance of various types of opportunities to keep up with developments, sharing new information in the institution, problems that might be experienced, advantages expected from using current awareness services, and interest in searching for solutions (e.g., through training interventions, access to current awareness services, e.g., through a Website, software solutions, or collaborative information seeking/work).
The following broad categories were covered in the interview with the centre staff: c hanging and dynamic working environments, importance of keeping up with developments, getting information, keeping up with developments, effectiveness of resources to keep up with developments, sharing information, problems experienced, and enthusiasm for using current awareness services.
Although the combination of methods was very useful and ideal for collecting information rich data, it needs to be adapted to accommodate busy and fairly inflexible schedules. The following are suggested (Fourie & Claasen-Veldsman 2007a:51):
The findings for this exploratory study are based on a qualitative analysis only. From the questionnaires and especially interviews, a few key issues were identified for further analysis. The identification of these is based on the guidelines by Gorman and Clayton (1985) and Williamson (2006) to identify main, recurring themes and supporting evidence supported by respondents' own words. For the moment a quantitative analysis will not be done, for example identifying correlations between the demographic data (e.g., age, gender, qualifications) and interest in current awareness services.
The demographic information was collected to get a clearer picture of the participating group. At this stage there does not seem to be any obvious correlations. From the total of twenty-six research participants, all of them were female, except for one male (the head oncologist). The age distribution of the participants is as follows:
| Age distribution | ||||||||
|---|---|---|---|---|---|---|---|---|
| 20-25 | 26-30 | 31-35 | 36-40 | 41-45 | 46-50 | 50+ | Total | |
| No. | 1 | 4 | 7 | 4 | 4 | 1 | 5 | 25 |
Respondents closer to retirement indicated that they might be less interested in current awareness services: 'At my age… too late to start with such things. My family is for me the most important'.
The academic qualifications of the participants ranged from Grade 12 (i.e., highest secondary qualification) to postgraduate qualifications (e.g., a Masters' degree in Social Work). The Sisters had a tertiary qualification (e.g., a degree in nursing).
With the exception of two, none of the participants had specific qualifications in oncology nursing, only work experience. Most had between one and ten years experience in oncology, while a few had more than twenty years experience, with the highest being twenty-five years. A wide variety of other experiences such as paediatric care, heart diseases, working in an old age home, and being a matron were mentioned.
We found that the daily tasks, as well as the institutional environment, have an impact on information-seeking behaviour and the need to use current awareness services. This includes the managing and financial environment, and the wider health care context. Although some of the patients treated by the two participatory groups overlap, there are considerable differences between the environment and settings in which the two groups (medical oncology centre and hospital wards) operate. Both are, however, affected by the South African health care situation, regulations and staff shortages, i.e., by the more comprehensive context. Kari and Savolainen (2007) stress the importance of context in information seeking for personal development. These publications as well as the Ingwersen and Järvelin (2005) model referring to social, systemic, work task, conceptual and emotional, economic, techno-physical, social and historical contexts, as well as the work of Lamb, King and Kling (2003) on organizational contexts, Menzies (1993) on the functioning of social systems as defence against anxiety and Strauss et al. (1985) on the social organization of medical work, should be used to guide data collection and interpretation in future research since these might help to explain the impact of anxiety, perceived roles and organizational dynamics on information needs and information usage that were noted. Suggestions are offered below (although these issues were noted, the paper will not, at this stage, pursue an in-depth analysis.).
The impact of surrounding environments is widely accepted (e.g., Courtright 2007; Wilson 1999a, b; Ingwersen and Järvelin 2005). The importance of considering the impact of the working environment (e.g., the difference between the medical oncology centre setting and the oncology hospital wards), as well as the perceived difference between South African and some other international health care environments (e.g., the UK or USA) was also specifically noted by the head oncologist: in South Africa, oncology nurses''responsibilities are much more' and there is 'Very scant emphasis on… academic development'. (Randell et al. (2009) note that nurses are expected to be more autonomous in the British National electronic Library for Health (NeLH).) It also seems from the exploratory study as if evidence-based nursing/medicine does not feature strongly in the South African context; this is an aspect that needs to be tested in further studies. The perception was also expressed that there is more emphasis overseas on patient research (at least in academic settings) than in South Africa. From findings mentioned in the following sections it also appears as if participants' perception of their role/function in the health care setting (e.g., receiving instructions and taking care of patients according to doctors' versus own input) can have an impact. In other settings in South Africa or in other countries it might, perhaps, be found that nurses have more responsibility in decision-making. From the survey it appeared that the nurses' own professional identity did not come through very strongly, but this does not necessarily imply that it does not exist. Unlike in the study reported by McCaughlin et al. (2005), they did not report the need for additional information in their decision-making, apart from what could be learned from the oncologists/doctors. According to them, nurses might have a perceived or actual lack of control over relevant factors.
The following briefly highlights some facets of the South African health care setting that may impact on the participants.
Pretoria , the setting for the empirical study, is one of the largest cities in South Africa with a number of oncology units and hospitals treating cancer patients. In Johannesburg (the largest South African city), about seventy kilometres from Pretoria, there are also a number of oncology units and treating hospitals.
Unfortunately the South African nursing situation is a concern for many: due to the long working hours and poor working conditions it is difficult to recruit staff and many young nurses are not staying in the profession for long: this is very similar to the situation reported by Menzies (1993). Nurses prefer to work overseas (e.g., in the UK, Ireland or USA) (Pienaar 2006). According to a report by Louw (2006), 42,000 nursing posts were vacant in contrast to the 41,563 posts filled.
At the time of the study, medical practices and hospitals experienced serious problems with regard to profit making from medication , due to new health legislation. This is still the case. Many had to cut staff and sometimes also had to settle for staff with lesser qualifications. Although inadequate funding is probably an international problem, it seems to have a serious impact in South Africa.
There are a number of cancer and oncology related societies in South Africa including The South African Oncology Nursing Society (no Website), The Oncology Social Work Association (no Website), The Cancer Association of South Africa, and the South African Oncology Consortium. Many participants were, however, not members.
More detail on the South African health infrastructure and regulations can be found at the National Department of Health Website.
The findings for the two settings (medical oncology centre and hospital wards) in terms of the environment are dealt with in the sections that follow.
The findings for the medical oncology centre are depicted in Table 3 and the hospital wards in Table 4 in the Appendix. It would be useful for further studies to explore different types of hospital wards such as academic hospitals and other private and government hospitals. (Suggestions are offered in the Recommendations, below.) The issues raised in Tables 3 and 4 also link well to findings by McKnight (2007) for inadequate time and support for literature searching and models of information seeking stressing the importance of the environment (e.g., Wilson's 1981 and 1996 models (Wilson 1999a, b)). Although anxiety resulting from not coping with the job was noted, this cannot at this stage be interpreted in terms of the work of Menzies (1991) and Strauss et al. (1985). Isikhan, Comex and Danis (2004) report on job stress and coping strategies in health care professionals working with cancer patients.
Menzies (1993) notes the following defensive techniques in a hospital environment confronted with anxiety:
In a medical environment Strauss et al. (1985:13) distinguish divisions of labour such as safety work, machine work, comfort work, articulation work and especially sentimental work. It seems worthwhile to analyse future work according to such divisions.
Information is mostly associated with effective decision-making, sense making, soothing anxieties experienced because of a lack of knowledge or a gap between what is known and what needs to be known, and problem-solving (Dervin 1999; Dervin and Nilan 1986; Belkin et al. 1982a, b; Wilson et al. 2002). Bearing this in mind a number of research projects have focused on the importance of information in the context of work, for example Byström (2002) and Vakkari (2003). Wessel et al. (2006) report on the link between the tasks of clinical research coordinators and their information-seeking behaviour . According to Byström (2002, 2005) there are tasks that are not information intensive and that are not related to problem solving. Different levels of information intensity can also be distinguished. The value and application of the task-based information seeking model is further explored by Järvelin and Wilson (2003). Li and Belkin (2008) also report on a faceted approach to conceptualising tasks in information seeking, exploring categories distinguished by various authors. The tasks of the oncology nurses are also mentioned in Fourie and Claasen-Veldsman (2007a), but are here, following a style of qualitative analysis, supplemented with quotes from the respondents' discussion.
A list of the typical tasks which the participants identified is included in Table 5 in the Appendix. As part of the exploratory study on which we are reporting it does not seem to be worthwhile to distinguish between the two settings or the position of the participants in terms of seniority and the level of responsibility they take (partly because we worked with a small and diverse group and the intention of the exploratory survey was to identify the route for more in-depth studies as indicated in the recommendations). It is, however, noted elsewhere in the paper that there are (as expected) higher expectations for the Sister-in-charge (medical centre) and the hospital ward manager to be able to offer information and guidance on completing tasks. Although we found considerable overlap between the daily tasks of the two groups in terms of their routine nature, there seems to be a difference between the intensity of some of the tasks and especially the extent to which patients rely on the nursing staff for information and emotional support.
There was strong agreement on the routine nature of their tasks and the fact that the nurses' main role concerns caring for patients, but without linking it to the need to use external sources to find information. No anxieties and stress to find information or information gaps were mentioned; if such occurred they rely on the oncologists and other doctors; only stress in taking good care of patients was mentioned:
Strauss et al. (1985) refer to sentimental work, and Menzies's (1993) defensive actions to deal with stress might be useful in further exploration. Respondents agreed that it is the responsibility of the oncologists to stay abreast of developments in patient treatment, and to ensure that they give nurses appropriate instructions. This is reflected in the following quotations from the interviews: 'Information can come from the doctor' and'I usually do what the doctors prescribe… for the doctors it is important [to access information resources], but not for me'. 'Not much is expected from them [the nurses] with regard to treatment' (The latter reflects the oncologist's as well as hospital unit manager's point of view). In contrast to this, respondents indicated that the oncologists are very busy and that they do not actually have time to share information. In further studies it might be worthwhile to test the validity of the oncologists as ultimate information source for all types of oncology related information, against the possibility of oncology nurses learning something from their own literature to successfully fulfil their daily tasks and functions, i.e., taking some responsibility in supporting the doctors. The question also arises whether the literature the oncologists/doctors monitor concerns nursing practices, or as one would expect, patient treatment and cure of the disease. Bertulis and Cheeseborough (2008: 187) note that nursing information is seen as patient- care centred and holistic in contrast to the medical and scientific information required by doctors, while Thain and Wales (2005: 133) found that searches by health care professionals were more related to patient care.
The well-being of patients seems to be at the centre of their work: 'I am a nurse and will always stay a nurse' (Sister) and'For me it is about the person - the patient' and'We do not have enough time for the emotional care of patients'. ' I think one actually shares a lot with these patients… because for them it becomes like a second home '. ' The reason why you studied nursing science was at the end of the day to get to the patients'. Being informed of developments and practices concerning patient education and emotional well-being might therefore help in at least patient education and counselling, and dealing with patients' questions based on Internet searches. Quotations from respondents also led us to the belief that a model for information behaviour in this particular health care sector should more strongly reflect affective (the need to emotionally care for patients) or affective-cognitive information needs (e.g., information on methods to deal with stress and anxiety) than purely cognitive information needs (e.g., the best drug to use for chemotherapy or dealing with nausea). The idea of emotional context is also mentioned by Ingwersen and Järvelin (2005) and needs to be further explored. A recent literature review showed that emotion features very scantly in studies on information behaviour reported in health care contexts (Fourie 2009).
When asked about the importance of the latest information we were told by a Sister: 'It will be nice to be oriented in such a way, but it is not essential'. Another explained: ' For me it is not that important… for the doctors it is very important. I usually do what the doctors prescribe'. It therefore seems as if the quality of the nurses' task completion does not depend on information for problem-solving or decision-making and as if their tasks are not information intensive: they can adequately take care of patients without searching for information. Nicholas et al. (2005: 40) also note: 'It was apparent that information seeking did not form part of the culture of the job, except with regard to training'.
The Sister-in-charge (medical centre) who takes more responsibility in supporting other staff members with information and who is also involved in conference presentations and research is the only one who occasionally uses the Internet, medical databases and tables of content as part of her job. The head oncologist also expects her to put in more effort to keep track of new developments. In a study with Bakker at the Central Cancer Library of the Netherlands Cancer Institute (still to be published), a respondent remarked that although some of them are very keen on keeping up with new developments, there are also some staff who do not even bother to look at the national professional journal.
Nursing staff from the medical oncology centre seem to take on more doctor-related responsibilities than the typical nursing activities that apply in the ward. They need to handle as many patient telephone queries as possible, before directing patients to the oncologists: 'she (a Sister) is the first step in the system… many of the things I do not even know about… only hear afterwards that this and this have happened… that the problem has been sorted out'.
Patient care is, however, not just about following instructions on treatment; there are many issues involved such as guidance, preparation, education and, especially, emotional care and support, as has been pointed out in the list of daily tasks and functions in Table 4: ' the questions people ask us, are often more emotional '.
Although it was not specifically investigated by the exploratory study, it seems as if information needs can also be influenced by staff members' positions (e.g., higher expectations for the Sister-in-charge and ward unit manager to be well-informed). This is an aspect that needs to be addressed in further studies.
Both groups mentioned that there is an increase in the number of patients finding information on the Internet: they ask more questions and have more sophisticated information needs. The nurses are concerned about this trend since they question the quality of the information the patients find on the Internet: 'The patients know more about the new things than me '. 'Patients very well informed about new things… it makes things difficult'. It was also mentioned that information on the Internet is not filtered: 'For some or other reason patients have more access to rubbish than access to things that are useful'. This also leads to feelings of inadequacy: ' One feels stupid if patients know more than you do because they went onto the Internet '. 'On quality it can become an issue, when someone asks you something and there stands the nurse and 'Er… um' . It therefore seems as if the need for patient information may be a good rationale for the use of current awareness services in an environment which appears to be mostly not information intensive. It might, for example, be very useful if nursing staff can identify and refer patients to appropriate information available on the Internet.
From experiences with this exploratory project (as will also become clear in the following sections) it seems as if there is a need to consider the use of current awareness services not only for factual information, for example on patient care and new job opportunities, and problem solving, but also for the affective dimensions of information, for example on joy, comfort, job satisfaction and inspiration. (McKnight (2007) also reported that the health care professionals cared deeply for their patients.) This seems important in professions such as oncology nursing, where not only physical care according to doctors' instructions, but especially emotional care features very strongly. Strauss et al. (1985) refer to sentimental work, while such care and emotions, according to Menzies (1993), lead to defensive actions, which might again be the cause of avoiding information. Considering the potential value of current awareness services for oncology nurses, the question arises whether research as reported in this article should merely note reported information behaviour, or whether expected changes in the future should also be considered. For example, the oncologist noted there is not a culture of information use: the nurses rely on their existing knowledge base and the oncologists. Somewhere in the future, this will probably prove inadequate. Bertulis and Cheeseborough (2008:186) noted that workplace culture (affecting information seeking) is as important as information technology.
Considering the work by Byström (2002, 2005) and Vakkari (2003) on task-based information seeking and the importance of considering the complexity and information intensity of tasks and functions, it is suggested that future collection of data (e.g., with the view to recommend current awareness services and Websites) should work from a preliminary categorisation of functions/daily tasks. Such a categorisation should also acknowledge categorisations from oncology nursing literature. With hindsight it seems as if the work by Menzies (1993) and Strauss et al. (1985) on the social organization of medical work and the defences in dealing with anxiety should also be noted, and used as bases for future studies.
Considering the models of, for example, Wilson (1999a, 1999b), Ellis (1989), Kuhlthau (1991, 1993), Dervin (1999), and Belkin et al. (1982) there is no evidence that the nurses are strongly aware of needs for information, gaps in their knowledge base, etc. that cannot be filled by the oncologists. There was also no mention of anxiety or uncertainty because of inadequate information. Considering the defensive actions by Menzies (1993), it was noted through personal observation that the nurses do not quite have the opportunity for splitting up the nurse-patient relationship (especially in the wards), but there seems to be a trend to reduce the impact of responsibility by delegation to superiors. To test whether the other defensive actions mentioned by Menzies (1993) apply and impact on information seeking, a follow-up study would be required. Considering the work division of Strauss et al. (1985) it seems as if the sentimental work category features strongly.
Apart from the routine nature of most tasks, participants especially stressed that their work is very tiring and emotionally demanding. More patients are, for example, dying than in the general hospital wards, which would, according to Menzies (1993), impact on defensive actions. They spend a lot of time on their feet, and, the hospital staff especially, work very long shifts (i.e., more than twelve hours per shift). All complained about numerous interruptions and the lack of privacy, which is seen as an inhibiting factor for effective information seeking. Due to staff and financial shortages, the hospital staff especially finds it difficult to participate in opportunities for continuing education, and to balance these with their responsibilities in their personal lives: 'Difficult to attend courses… difficult to get out of the wards… do not want to come in on my day off'. Apart from the fact that their daily tasks do not require them to search for information, they do not have the time and energy for information searches:
Similar concerns and the lack of time for information searches were also noted by McKnight (2007).
Current awareness services appropriately planned and tailor-made according to individual preferences can, however, be a great time saver, as we will explain in our recommendations. However, because most participants were not familiar with the concept of current awareness services, this is something that they do not realise, and that needs to be demonstrated. When promoting the use of current awareness services, it seems as if there should also be a strong consideration of the demands of people's jobs. Current awareness services pushing information to nurses is also supported by Randell et al. (2009).
In spite of opinions that they do not need to seek additional information to complete their daily tasks, some remarks pointed to an interest in information, e.g.
We questioned management as well as the nursing staff on their perceptions of influences and barriers to the use of information and Internet current awareness services. These should be read against the impact of the environment and daily tasks as already discussed.
Staff from the medical oncology centre felt that they did not have enough time and private access to the Internet to use current awareness services. Due to the routine nature of their daily tasks, there appears to be no real need for them to look for additional information. Most of them lacked computer skills as well as skills in using the Internet (this seems to be a major barrier). Nicholas et al. (2005: 39) also noted poor access to computer facilities and not enough networked terminals, and perceived low levels of Internet literacy and awareness.
The Sister-in-charge, however, felt confident about her skills. She is also the only one who is currently using some current awareness services (e.g., tables of contents to which the oncologists subscribe and occasional database searches when necessary). She also regularly presented papers at conferences.
From management's point of view, the centre staff did not require additional information to complete their tasks. It was also mentioned that they might not always see the value of information for their tasks, and that many lack personal motivation or reasons for spending time on information seeking: 'depend on individual interest… for many just a job… not an academic approach' ;'milieu is not there to work in such a way' and 'you must have the opportunity as well as the reason to use it'. Bertulis and Cheeseborough (2008: 187) found a relationship between employer attitudes to evidence-based practice and the ability to access electronic resources at work. They also noted that the level of encouragement by organizations and perceptions of whether they have time for information seeking is important.
The hospital staff claimed lack of time, the physical and emotionally demanding nature of their jobs, inadequate funding and access to the technology, as well as the lack of opportunities as barriers to the use of information and current awareness services. They especially lack computer skills and skills in using the Internet, and the opportunity to use the Internet. The unit manager thought they could perhaps 'create a little corner…where those who are really interested… perhaps in their time off ' (referring to lunch breaks) could use the Internet. It was also mentioned that the nursing staff lack knowledge of oncology issues, and that training opportunities are limited: 'Not really us who get the opportunity to do it'
Although they were all aware of the Internet, most do not know how to use it. One nurse said about the Internet: 'I just heard about it'. Only one participant has received formal training in information searching as part of her university studies. These barriers were also raised from the hospital management's perspective.
One nurse indicated that she has access to a laptop at home, but that she does not really know how to use it and, therefore, does not use it for e-mail or access to the Internet. A link between computer skills and an inclination to use electronic information sources is also reported by Secco et al. (2006).
One of the very few who feel confident about her search skills said. 'Oh no, I'll find it… I'll find it… no matter… I'll find it… OK… I'll get it'. Most felt less confident: ' If I try to search something, I battle… I am scared that I will waste time and money, because I do not actually know how to search '. Also: 'If somebody asks me something, I will ensure that he gets the right information, but I will not spend the whole day searching for it'.
Tannery et al. (2007) and McKnight (2007) noted similar barriers of lack of time, lack of access to information resources and lack of skills. The possible impact of personal characteristics and attitudes, adoption of innovation, and lack of professional curiosity are also mentioned by them.
From the study it was also clear that nurses cannot afford to stay abreast of their subject field and enrol for events of continuing education if not supported financially as well as in terms of time allowed.
As stressed before, both the nurses and management feel that information is not essential to successfully complete their daily tasks. In cases where they need to know something they consult with the oncologists, Sister-in-charge, ward unit manager or other senior staff members. Staff from the medical oncology unit are expected to at least be aware of what is reported at South African conferences.
There was general agreement that the oncologists are very up-to-date, and that they make every effort in this regard. They are, however, considered to be less successful in sharing information with the nurses. Due to the fact that they try to keep up with developments, the oncologists are also well aware of the negative effects. One respondent, however, stated'I think they do it (sharing information) quite well'. With regard to book announcements it was remarked: 'people force information down from a company's perspective'. They can only consider'what you have time for… 90% I never look at'. One participant mentioned interest in medication: 'Maybe about the research they have done' (she was planning to enrol for a qualification in oncology nursing). Tannery et al. (2007: 18) mention the following as a barrier: 'Did they perceive cues in the environment that discouraged the use of these resources, such as disparagement from supervisors or a perception that consulting the professional literature during work hours is wasting time?' This issue was not explicitly stated in this study.
On the value of current awareness services and the information obtained, the following views were expressed:
In spite of the barriers that were raised, these statements leave the impression that at least some of the participants could see the benefit of keeping track with information. From a management perspective it was explained: 'Since there are so many changes in oncology one must really stay abreast of all the developments… I think we have a large gap for this… working under so much pressure''it is as if we get stuck on the same type of stuff'.
Participants were mostly unaware of current awareness services, and therefore also of how this can be used in their jobs. This might be in contrast to other settings. A study in 2009 in a different South African context showed more interest in the use of information and current awareness services, while the previously mentioned study in The Netherlands noted that not all staff are keen on using information or current awareness services.
In South Africa all nurses have to be registered with the South African Nursing Council. Some of the nurses are also members of The Democratic Nursing Organisation of South Africa (Denosa). Very few participants were, however, members of national professional societies (e.g., The South African Oncology Nursing Society and The Oncology Social Work Association). They had hardly any knowledge of the international societies or the information that can be gained from these societies' Websites (e.g., newsletters, conference announcements). One also said that she did not ' know where you can buy new books' while others indicated that they are only aware of books brought to their attention by Denosa. None of them used discussion lists as a means of keeping up. The oncologist felt that such information is often sufficiently covered by formal sources. Even some of those with their own access to the Internet and computer skills did not often use it for information seeking: 'I am scared I will waste time and money'.
Although the medical centre subscribes to professional journals, these are not necessarily aimed at oncology nurses. The hospital staff had no access to the professional journal literature or tables of contents. Both groups indicated that they take note of conference announcements and opportunities for continuing education (mostly locally). (We did not attempt to determine whether they noted all important/key events.) None of the respondents was using discussion lists, RSS feeds, online tables of contents and tables of contents services, Weblogs, Web monitoring services, news alerting services or Web portals. Except for the Sister-in-charge (medical centre), most do not have the skills to use these. They are also unaware of the variety of current awareness services available for free (e.g., as identified by Fourie & Claasen-Veldsman 2005, 2007b), or how this can help them to actually save time and improve the quality of patient care. Although there seems to be a serious lack of computer skills, somebody mentioned that management expects them to read the protocols (for administration of medication) on the computer. They should not print it out.
A few participants mentioned that they sometimes receive useful information from patients, most often such information is, however, considered to be unreliable due to the poor reputation of Internet information sources: 'Tons of information available from the Internet - they don't know what to do with it… Patients argue with doctors about information they found on the Internet… they do not believe the doctors'. In an earlier study, Fourie and Claasen-Veldsman (2005, 2007b) identified some very useful resources that are aimed at patients. By using current awareness services nurses can, for example, notice such resources and bring them to the attention of patients.
Other preferred sources of information are colleagues, reference works, conferences and workshops. The last two are especially highly valued as means of continuing education and keeping up with developments. The oncologist also confirmed that excellent formal training opportunities are presented at conferences. Although there seems to be trust in relying on colleagues for correct answers, it was also confirmed that there is not a strong culture in sharing and disseminating new information: senior staff members who are more exposed to new information just do not have time for this. 'I am willing to share information as long as they do not pick my brain'. 'I almost do not get the opportunity, because there is not time… to give feedback to the staff'. Earlier work by Sonnenwald (1999) on horizons would be useful to further explore their use of information resources with a strong reliance on doctors and colleagues (mostly senior).
In spite of the fact that there is no obvious need for information to complete their daily tasks, and the barriers we have noted, many participants indicated that they would be interested in learning about current awareness services, and especially in learning computer and Internet search skills. Staff members who are ambitious to further their careers, seemed especially interested in using current awareness services, while staff members who are very close to retiring age felt that they would rather focus on'being a nurse - caring for patients' and using their personal time for their families. When asked about attending a workshop we heard:
Others indicated less time, such as four or six hours, for attending a workshop, and some also pointed out the practical realities such as it would'depend on day', and their shift. 'Maybe in a month you can go twice' (two hours at a time).
About using their personal time for current awareness services one respondent remarked: 'Must get away from the situation', and about access: 'outside the job/work situation there are many Internet cafes'.
Although staff are not expected to use current awareness services, management from both groups indicated that they are interested in exploring further the possibilities current awareness services could offer to their staff and that they would support staff in attending a workshop in using current awareness services. For most participants, a workshop in computer skills would, however, be a pre-requisite. (Their interest in learning information technology skills could be further explored, for example, by considering educational literature and literature on adult learning. It was mentioned that if they do not develop a culture of using current awareness services, staff will continue to rely on'a past-base' (i.e., based on knowledge gained in the past) which at some point in the future will no longer be adequate. We 'need to create a milieu for training, research… in comparison with clinical work time'.
With regard to support from the hospital management: 'I think they can improve considerably on the support'. There are, however, opportunities for personal development in the hospital, for example for computer literacy training. 'They must create an opportunity, or give a reason, why not'.
Overall the participants were interested in receiving information on medical and drug related issues, job and training opportunities as well as information for personal use. For example, they would like to use the Internet to help their children with their homework, and to impress their children. Putting in the extra time to learn search skills might thus have a double benefit. In spite of their interest, participants were not quite sure how they would use it, or how they would find the time: as mentioned before, they did not seem to realise that current awareness services that are based on push technology can actually save time in contrast to one-off information searching. Therefore, we will interpret their interest as conditional interest: the use of current awareness services and the training should be streamlined and tailor-made to meet their needs and circumstances.
In addition to what has been mentioned, the work by Vachon (1998) on personal coping strategies in palliative oncology settings, which explores the need to find pleasure in one's professional role and experiencing a feeling of accomplishment, should also be addressed in further exploration, as well as the development of interventions. 'Association in a professional interest group may be particularly helpful to caregivers who do not receive the validation they need in their particular work setting' (Vachon 1998:154). This should also be aligned with the work of Menzies (1993) on the functioning of social systems as a defence against anxiety, and research following on her work, e.g., Van der Walt and Swartz (2002) on task oriented nursing in a tuberculosis centred programme in South Africa.
Stokes and Lewin (2004) used soft systems analysis to depict the information seeking behaviour of nurse teachers that is neither precise nor predictable, as a rich picture. This followed the work of Checkland (1999). Figure 1 presents an attempt to apply this to this study with the intention to show the potential for in-depth application for future studies and for building a theoretical model in future, adding insights gained from other studies.
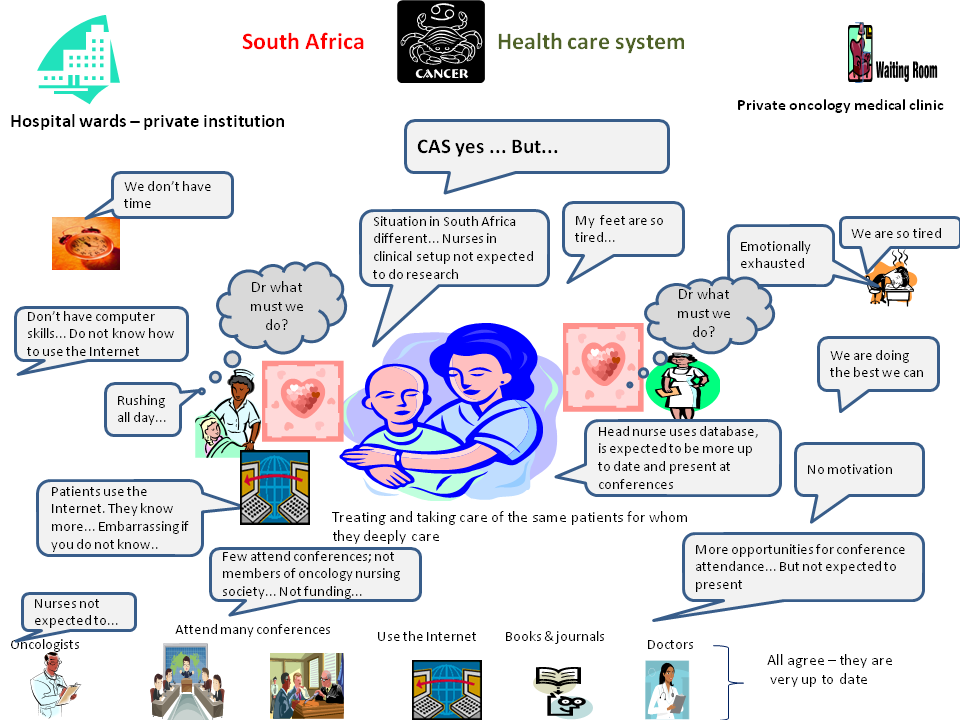
Table 6 (in the Appendix) depicts the potential of force field analysis to identify the strengths and weaknesses of the research setting towards the use of current awareness services. Force field analysis is a technique for implementing changes in structure, technology and people, and can identify three sets of organization field conditions, namely facilitating, constraining and blocking. The technique was developed by Kurt Lewin in 1951 and since then has had many applications, e.g., Ajimal (1985), Thomas (1985), Baulcomb (2003) and Cronshaw and McCulloch (2008). In this paper it will only be presented to show the potential of the technique for future studies.
The study reported here involved only a small number of oncology nurses in a specific setting. It might be that findings in some regards might differ when considering other settings. Considering the fact that neither of the South African professional societies / organizations for oncology nurses and social workers had a Website at the time of writing, it seems safe to assume that much needs to be done to promote the use of current awareness services available via the Internet by oncology nurses in South Africa. Apart from depicting the findings using a soft systems approach, the limited scope of the study does not quite lend itself to suggesting a model of information behaviour regarding current awareness services at this stage. Recommendations to move forward in this regard are, however, offered.
Some practical recommendations are mentioned by Fourie and Claasen-Veldsman (2007a). The intention of this article, following a more in-depth analysis was to note the methods, theories and models to explore in future studies.
We acknowledge the impact of the environment and daily tasks on the oncology nurses' information needs, and the fact that many tasks are not information intensive. In the light of the changing demands of society and the increased use of the Internet by patients, we however feel that we need to further explore the potential of current awareness services and information dissemination and move beyond the barriers that have been mentioned. A soft systems analysis, force field analysis and Roger's theory of diffusion seem useful to deepen understanding of the context and promote a culture of using current awareness services. In addition, anxiety to give patients the best possible care, as well as a strong shift towards the oncologists and other doctors were noted in the responsibility for decision-making and staying abreast of developments. Future studies may thus benefit from working from the defensive actions against anxiety as identified by Menzies (1993) and the division of labour identified by Strauss et al. (1985).
Following the force field analysis depicted in Table 6 (Appendix), we recommend that the following should be in place in order to promote the use of Internet current awareness services as information resources for oncology nurses:
For further research we recommend the following:
Although the sample group of oncology nurses for the exploratory study had hardly any knowledge of Internet current awareness services, and although there are many barriers to information seeking, it seems as if there is an interest in promoting a culture of using current awareness services. In order to develop an appropriate current awareness service infrastructure and training opportunities and other interventions tailor-made for the needs of oncology nurses, we need to deepen our understanding of the information behaviour of oncology nurses and their context. This implies that we take note of the information seeking behaviour of other health care professionals as well as cancer patients, and that we expand our survey to accommodate national and international comparative studies.
To gain real depth in our understanding we intend to develop a preliminary th eoretical model for the use of current awareness services by using the results from the exploratory study, re-interpretation of the results against a selection of existing models (e.g., Lamb, King and Kling's social informatics and Rogers' innovation and diffusion model), as well as an extended literature survey to identify other ways of looking at information behaviour and exploring context. Such a model can then be tested.
Our thanks to the anonymous reviewers for bringing the publications of Menzies and Strauss to our attentionand to to Mrs Joukje Geertsema for her help with the conversion to HTML format.
Ina Fourie is a full professor in the Department
of Information Science, University of Pretoria, South Africa. She
received her Bachelor's degree in Library and Information Science,
her Honours and Masters degree in Library and Information Science
from the University of the Orange Free State University,
Bloemfontein (South Africa) her D.Litt et Phil from the Rand
Afrikaans University, Johannesburg (South Africa), and a
Post-graduate Diploma in Tertiary Education from the University of
South Africa (Pretoria). She can be contacted at ina.fourie@up.ac.za
Retha Claasen-Veldsman was a junior lecturer in the Department of
Information Science, University of Pretoria, South Africa at the
time of writing. She obtained her qualifications, a BA Information
Science, BA (Honours) Information Science and an MA in Development
Communication from the University of Pretoria. She currently work
for GEM-Science as public participation practitioner. She can be
contacted at info@gemscience.co.za
| Find other papers on this subject | ||
| Autonomy | Privately owned by a group of oncologists. They make their own decisions with regard to the infrastructure, staff appointments, staff duties, the budget including subscription to information services, conference and workshop attendance, etc. They can make their own decisions on introducing current awareness services to the nurses and other staff members. |
| Financing | Reasonable funding (including sponsorships from industry) is available for continuing education, current awareness services, conference attendance, etc. The oncologists frequently attend international conferences and make use of other opportunities for peer interaction. Staff members on other levels (e.g., the nurses, social worker, pharmacists) also get opportunities to attend conferences, courses, workshops, etc., nationally as well as internationally. Although it is recommended, they are not expected to do presentations or to publish. |
| Infrastructure | Although computer and Internet access are available to the staff (management felt the number of computers to be adequate), not all staff members have individual access. Some pointed out the lack of privacy and opportunity for uninterrupted searching. (They felt that a dedicated computer in a separate room might be a solution.) In cases where it was essential for their daily tasks (e.g., the Sister-in-charge and the social worker), they did, however, have their own computers. |
| Staff situation | The centre relies on the support of a multi-disciplinary team including the Sister-in-charge, oncology nurses, a social worker, pharmacists, financial and administrative staff. They receive their instructions from the oncologists and rely on them to keep up with new developments. For some aspects they rely on the Sister-in-charge. The staff is mostly expected to work conventional office hours. However, they feel that the work is very exhausting, especially since they spend a lot of time on their feet. |
| Patients | Although most patients are from Pretoria and surrounding areas, there are also patients from elsewhere in the country. Only some of the patients are hospitalised. Interaction with patients in the centre seems to be less intensive than in the hospital wards: they come to the centre for shorter periods (e.g., an hour or a few hours at a time), or even shorter periods for consultation only. |
| External pressures | The centre is experiencing pressures due to the South African National Health Act (Act 61 of 2003) and the Government's health policy. They need to ensure that they are nationally and internationally competitive, that they are involved in research, and that the oncologists keep abreast of developments (e.g., through conference attendance, monitoring the professional literature, as well as membership of professional organizations and other bodies). Due to the nature of their tasks, the oncologists have a strong sense of the importance of current awareness services; they are active users of a number of them. There is, however, no evidence that other staff members experience similar pressure. |
| External interaction | Interaction with other national as well as international institutions, medical practices, professional bodies etc. is considered very important, especially for the oncologists. |
| Autonomy | A unit manager (rank of Sister) is in charge of the two hospital wards. She reports to the hospital management. The hospital is privately run and forms part of a large South African hospital group. Although the unit manager and nursing staff may make suggestions on continuing education, IT infrastructures, etc., these need to be approved by the hospital management. The hospital staff must follow the oncologists' orders for patient treatment. ('They take orders and we [the oncologists] must come up with the orders'). If they want to promote the use of current awareness services, they will need permission from the hospital management, especially if funding is involved. |
| Financing | Considerably less funding and opportunities than for the medical oncology centre are available for continuing education, conference attendance, etc. It was mentioned by participants that it is often only the senior staff that receive such opportunities. There are, however, some opportunities available for everybody as part of the staff development programme. |
| Infrastructure | There is one computer with e-mail access available in the wards. This is used for administrative purposes. Participants (including the ward unit manager) felt that this is inadequate. Internet access is only available for the hospital top management. |
| Staff situation | There is a clear hierarchical structure, including the ward unit manager, Sisters, nurses, staff nurses and assistant nurses as well as care workers. They are experiencing serious staff shortages, and work very long shifts (more than twelve hours per shift), with a lot of time on their feet. They are not expected to keep up with new developments concerning the treatment of cancer or the administration of medication, chemotherapy or drugs. This is the oncologists' responsibility. There is also very little emphasis on academic development: their main function is to care for patients to a very high standard. They have day and night shifts. (For reasons of convenience, we only included staff working the day shift in our survey.) It was, however, mentioned that the circumstances of the night shift may differ; patients, for example, ask more questions during the day. 'More questions during the day than at night… see them for two hours and then they sleep… less time to chat'. 'Day shifts are completely different from night shifts'. (Translated from Afrikaans.) |
| Patients | Staff only interact with the centre patients who are hospitalised, often for periods of several weeks. The interaction with patients therefore seems to be different from that of the centre staff. (This is explained in more detail in the section on tasks and functions.) It also seems as if there is more opportunity and need for (potentially information rich) interaction with patients and patient education, an issue that we will raise again in the recommendations. |
| External pressures | The hospital is experiencing pressures due to the South African National Health Act (Act 61 of 2003) and the Government's health policy. The quality of the care they offer should meet with the expectations of the oncologists, patients and the hospital management. |
| External interaction | There is less pressure for interaction with other national and international hospitals and organizational bodies. Some of the hospital staff does, however, have informal contact with staff from other hospitals. The ward unit manager admitted that she and other hospital staff do not experience the same pressures as the oncologists to be competitive. |
| Tasks | Comments |
|---|---|
| Administration of treatments | This includes chemotherapy, assisting patients with hygiene, wound-care, and injections. Although treatment is offered by both groups, the treatment of hospitalised patients is often much more intense and more intensive, for example, chemotherapy for eight hours a day over a period of five to six days. All treatment is prescribed by the oncologists: the nursing staff must merely ensure that it is correctly and appropriately administered. The perception is that the responsibility to keep up to date therefore lies with the oncologists, and not the nursing staff. (In other settings and countries it may be that the nurses may have more responsibility for taking decisions.) |
| Monitoring and observation | This includes monitoring, for example, blood pressure, weight, blood results, and fever, with appropriate and regular feedback to the treating oncologists who take responsibility for appropriate treatment. |
| Administrative tasks | At the centre these include patient admission, patient appointments, getting results of tests, ward bookings, charging accounts, telephone enquiries, reception management, switch board management, the organization and preparation work for stem cell transplants and the management of patient records. |
| Staff management | This includes the delegation of tasks and staff management, and was specifically pointed out by the hospital staff. |
| Doctors' rounds | A senior hospital staff member needs to accompany the oncologists on their rounds with patients. This often happens twice a day at times that fit in with the different oncologists' schedules. |
| Information sessions | The hospital staff needs to lead and participate in information sessions at shift take-over. They, as well as staff from the centre, are also expected to attend meetings by the oncologists where information on patients is shared. |
| Patient education and counselling | Both the hospital and centre staff saw this as an important function. It includes sharing information with patients, for example on self-treatment such as self-injection and the implications of treatment processes, preparing patients for stem cell transplants or aftercare, and answering routine queries. The social worker and the hospital staff also mentioned counselling and emotional support for patients and their families: 'They always look to us for answers' and'Our patients need a lot of emotional support, because they are very ill'. 'Talking to the patients… giving them guidance on the illness'. 'They like contact with patients'. (The latter is a translation from Afrikaans from the interview with the oncologist.) |
| Daily physical care | The hospital staff must ensure, amongst other things, that patients receive their meals, exercise where necessary, and that their beds are made. They also need to offer advice on dealing with nausea, vomiting, etc. |
| Staff training | The hospital group need to offer in-service training for new staff members. |
| Support of hospital staff | This is mostly the duty of the care workers who need to help with the washing and feeding of patients when necessary, as well as helping with other small tasks for patients. |
| Working with children | One of the hospital wards specialises in the treatment of children. They stressed the fact that paediatric care has its own unique demands. 'Paediatric oncology… completely different'. 'A child is totally different from an adult under circumstances of illness' (Translated from Afrikaans.) (A participant responsible for paediatric care stressed her absolute reliance on the oncologist specialising in paediatric care for information.) |
| Facilitating | Constraining | Blocking |
|---|---|---|
| Well-being of patients is central in their work | Very few with formal training in oncology nursing | Lack of time |
| Growing interest amongst patients to use the Internet and confront nurses with information found | Do not have a culture of sharing & disseminating information | Lack of privacy |
| Care for patients central in their work | Do not have a culture of information use | Too many interruptions |
| Interest in using CAS (conditional) | Lack of confidence in finding information and using the Internet | Lack of access to ICT and the Internet |
| Strong confidence in ability to find information (unfortunately only a very few) | Task completion seem not to depend on information; tasks seems not to be information-intensive | Little emphasis on academic development |
| Strong affective and caring atmosphere and attitude | Work is emotionally tiring | Inadequate computer skills |
| Difficult to find a balance between emotionally laden work and personal life | Inadequate skills in using the Internet | |
| Focus is on clinical tasks and not research | Lack of funding and time for continuing education (specifically in the hospital wards) | |
| Information considered as'nice to have' | Lack of awareness of information needs | |
| Evidence-based nursing practices not strong in the country | Not required to search for information in their task completion | |
| Lack of formal information literacy and Internet search training | Do not have a strong professional identity - very heavy reliance on doctors | |
| Lack of motivation | ||
| Routine nature of tasks - main role is caring | ||
| Lack of time of oncologists to share information | ||
| Fair to considerable work experience in oncology nursing (this can be facilitating or constraining, but seems constraining in the contexts studied) | ||
| Trust in colleagues |
|
|
© the authors, 2011.
Last updated: 24 August, 2011 |
|
